
Here’s another EKG to get you guys talking. Thank you Dr. Silverberg and Dr. Brown for the case.
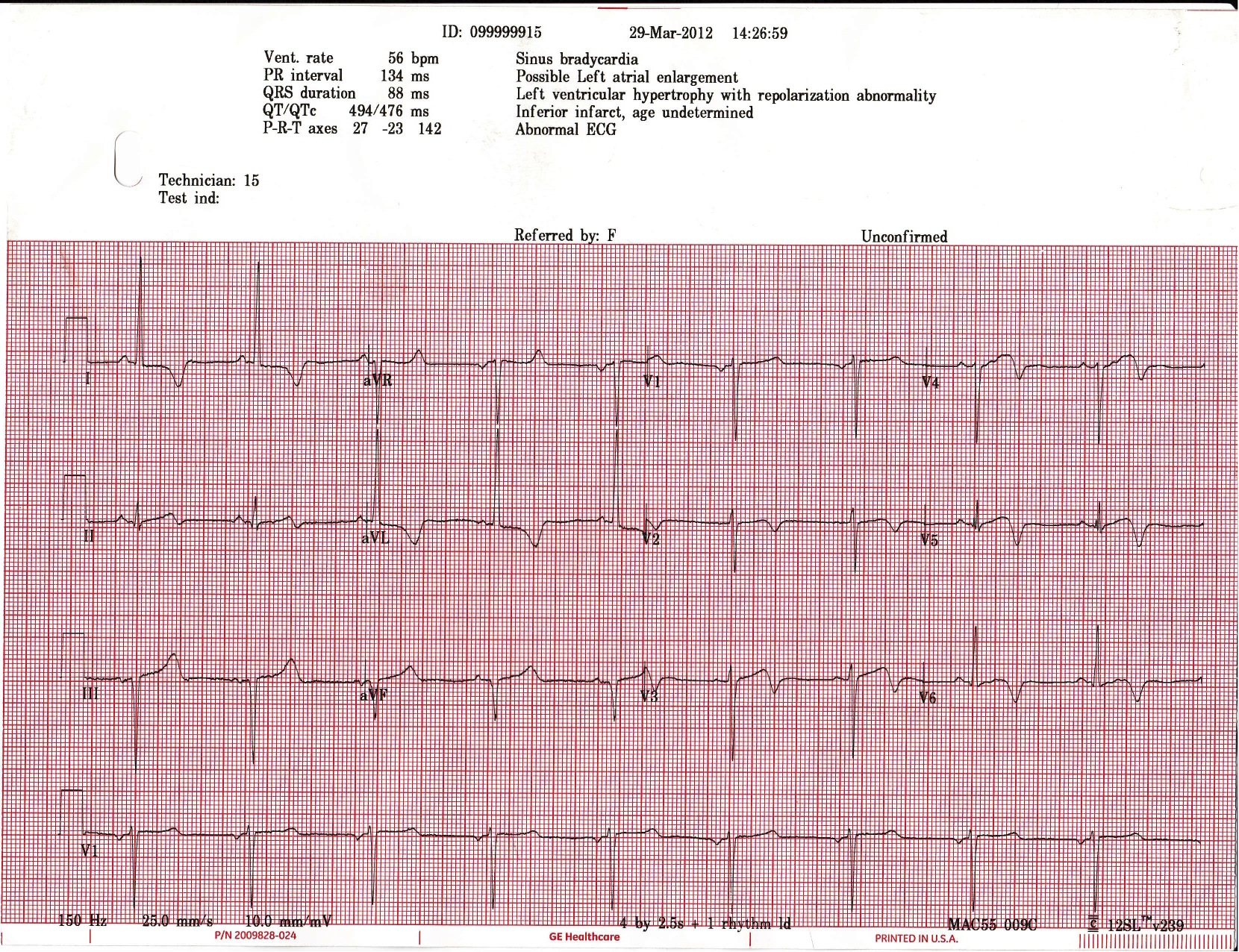
73 chinese female h/o dm, htn and high cholesterol had syncopal episode. Felt heart racing and palpitations prior to passing out at bingo in her church. Only complaint now is slight chest pain that is similar in nature to what she felt prior to today’s syncope only it was worse then. Vitals: hypertensive but the rest normal including the physical.
What’s the diagnosis?
What’s your management?
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

jwillis
James Willis, MD. Assistant Program Director at SUNY Downstate / Kings County.
Latest posts by jwillis (see all)
- Bedside Teaching - June 11, 2015
- How to Give A Lecture - February 12, 2015
- See One, Do One, Teach One: What Do EM Learners Want? - August 28, 2014
- Wednesday Wrap-Up - November 14, 2012
- Wednesday Wrap-up 8/1/12 - August 2, 2012
4 comments for “EKG 2”