
So in this week’s ICU conference EMS calls in for a notification that there is a 55 yo woman comes in who has a HR of 173, BP 140/91, RR 22, PO2 99% T of 100.1 with multiple AICD discharges. It was a great case with a great EKG. After further investigation we sent off a thyroid panel and you see that the TSH is undetectable. So now that you have your diagnosis, what is your treatment algorithm?
Typically in the ED we often do not formally go over these scoring systems but Burch and Wartofsky developed a point system based on multiple organ systems with diagnostic parameters which are below.
Thyroid Storm Classification
| Diagnostic parameters | Scoring points |
| Thermoregulatory dysfunction | |
| Temperature °F (°C) 99–99.9 (37.2-37.7) 100–100.9 (37.8-38.2) 101–101.9 (38.3-38.8) 102–102.9 (38.9-39.2) 103–103.9 (39.3-39.9) >/= 104.0 (>/= 40.0) |
5 |
| Central nervous system effects | |
| Absent Mild (agitation) Moderate (delirium, psychosis, extreme lethargy Severe (seizures, coma) |
0 |
| Gastrointestinal-hepatic dysfunction | |
| Absent Moderate (diarrhea, nausea/vomiting, abdominal pain) Severe (unexplained jaundice) |
0 |
| Cardiovascular dysfunction | |
| Tachycardia (beats/minute) 90–109 110–119 120–129 130–139 >/= 140 |
5 |
| Congestive heart failure Absent Mild (pedal edema) Moderate (bibasilar rales) Severe (pulmonary edema) |
0 |
| Atrial fibrillation Absent Present Precipitating event Absent Present |
0 0 |
Scoring system: A score of 45 or greater is highly suggestive of thyroid storm; a score of 25–44 is suggestive of impending storm, and a score below 25 is unlikely to represent thyroid storm.
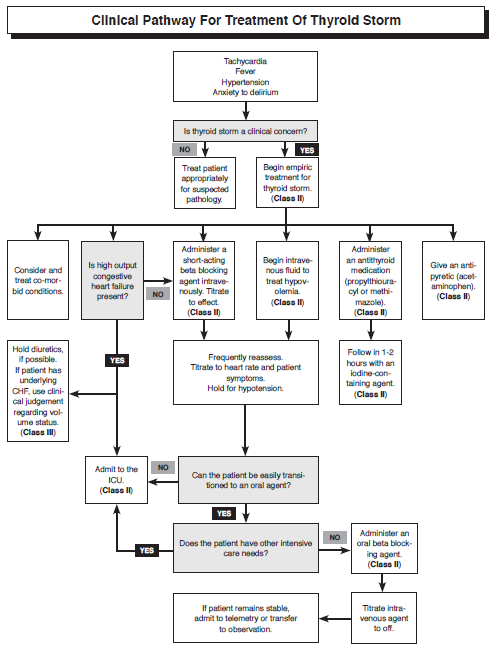
So you calculate that this person meets criteria for treatment of Thyroid Storm, What is the treatment?
Supportive care:
By now I know you have all established your ABCs.
Correct electrolyte abnormalities and give them fluids, preferably D5 containing substances. Hyperthyroidism is a hypermetabolic state and the patient is utilizing a tremendous amount of energy while they are in storm.
Control hyperthermia by external cooling and Tylenol.
During your treatment algorithm it is important to also look for signs of infection including drawing blood cultures and urine cultures, UA and CXR and treat accordingly because thyroid storm could be initiated by an infectious process.
Beta Blockers: with a special preference to propranolol which is an antiadrenergic that you can give po or IV and has the added benefit of preventing conversion of T4 to T3. But consider starting a beta blocker drip if your patient is not responding and especially if your patient is suffering from high output cardiac failure.
Propranolol: 1-3mg max rate of 1mg/min. Repeat only once after 2 minutes. Can start infusion at 2-3mg/hr
Labetalol: 5-20mg IV over 2 minutes then 0.5mg/min
Esmolol: Loading Dose: 500mcg/kg over 1 minute (70kg=35mg) Maintenance is 0-200mcg/kg/minute(70kg=0-14mg/min)
High Dose Propylthiouracil or Methimazole
PTU is the preferred agent for treatment of thyroid storm, it works faster, and it will prevent peripheral conversion of T4 to T3. It is loaded with 600mg – 1000mg orally, then 200mg to 300mg orally q4-6h max 1200mg per day
Methimazole is 20mg orally or rectally q4h
Glucocorticoids: will decrease peripheral conversion of T4 to T3 and may also be useful to prevent relative adrenal insufficiency due to hyperthyroidism.
Dexamethasone 2mg IV q6h or Hydrocortisone 100mg IV q8h
Iodine: give this po or og but must be given at least 1h after PTU administration
Lugol solution or Potassium Iodide 6-8 drops every 6-8 hours or contrast dye 600mg IV every 12h.
Plasmapheresis: is rarely needed but this will literally take out thyroid hormone that is bound to the proteins in the plasma and replace it with normal plasma. Contact Hematology.
References
Mills, L, Lim,S. Identifying and Treating Thyroid Storm and Myxedema Coma In The Emergency Department. Emergency Medicine Practice August 2009 Volume 11, No 8
Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am 1993;22:263–77
Richard.Shin
Latest posts by Richard.Shin (see all)
- Adult Journal Club 4.23.2014 - April 21, 2014
- Journal Club: Droperidol vs Haloperidol - March 21, 2014
- Just another COPD exacerbation or a PE? - July 24, 2013
- ICU Critical Care: Thyroid Storm - June 14, 2012
- Wednesday Wrap-Up: Pediatric DKA 4/4/2012 - April 4, 2012