
Here’s the answer to our last EKG!
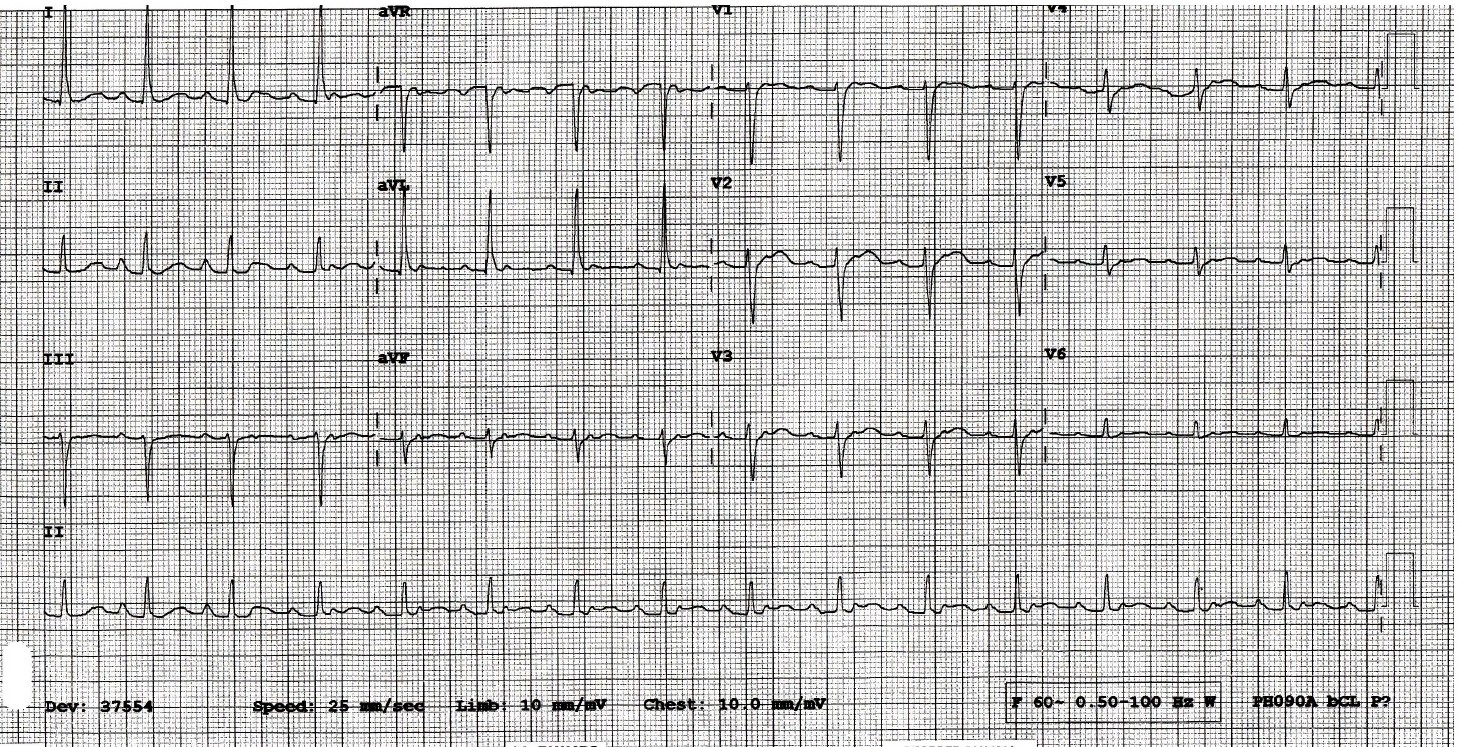
The major finding in this EKG is the abnormal rhythm. Looking at the rhythm strip (II) the patient starts out in sinus rhythm. Then after the 4th QRS we start to see additional p-waves. The rest of the rhythm strip shows an ectopic atrial tachycardia with a 2:1 block. Other than this finding the rest of the EKG shows normal QRS axis, rate just below 100, LVH (avL > 12mm).
This patient had presented multiple times with similar symptoms and had other EKGs shown below:
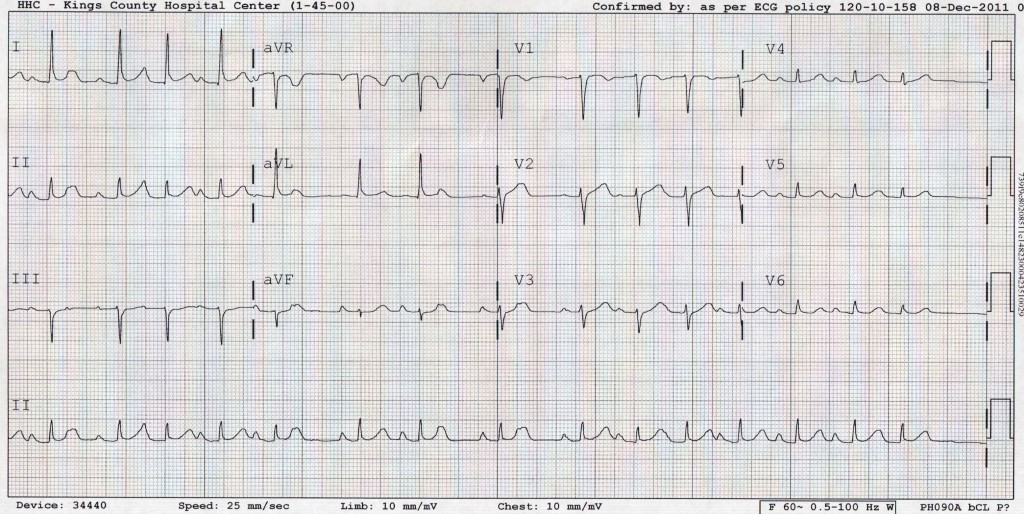
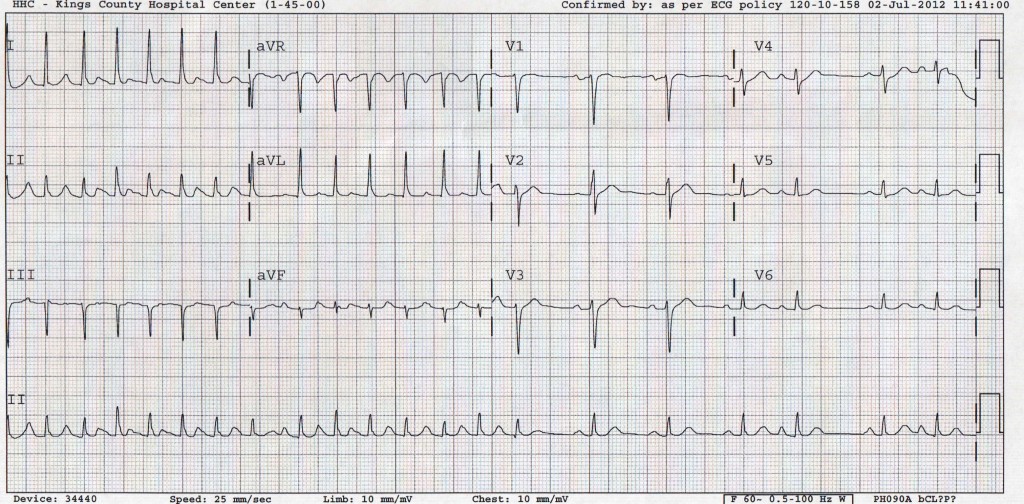
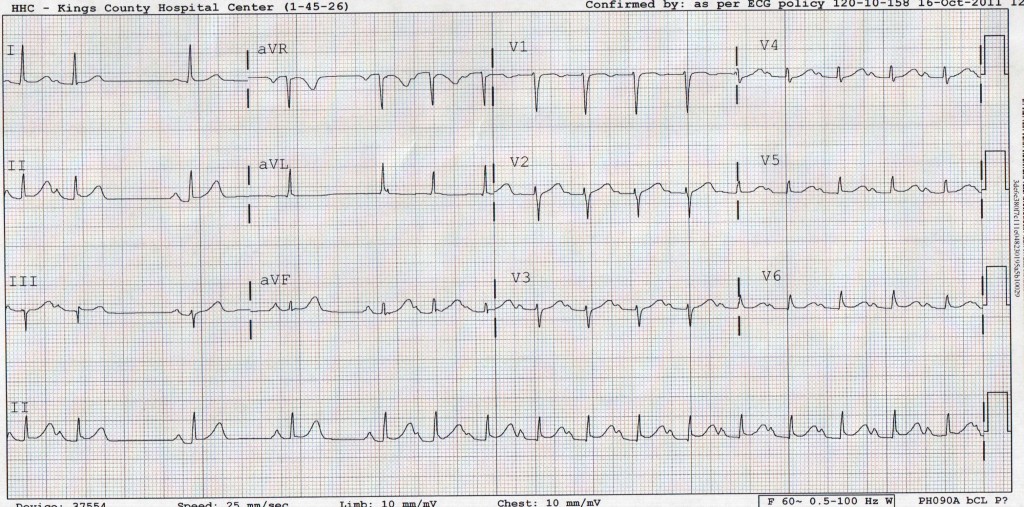
While none of these other EKGs show a block, they do show irregular R-R interval and the variable P-wave morphology. The irregular R-R can easily confuse most EKG machines causing them to label these EKGs as atrial fibrillation. However, we can clearly see P-waves before each QRS in these EKGs.
Given the findings of the initial EKG, it is important to distinguish Ectopic Atrial Tachycardia from Atrial Flutter. Often, Ectopic Atrial Tachycardia is mistaken for atrial flutter because of the multiple P-waves with variable conduction. However there are some specific EKG findings that you can use to differentiate them:
Atrial Flutter
- Rapid and regular rate ranging from 150-400 bpm
- Each flutter wave is followed immediately by another flutter wave. This is because the impulse creating the flutter is a re-entrant circuit. Once the circuit is complete, it re-activates itself. Thus, there is no isoelectric period between P-waves
- The classic sawtooth pattern is best seen in leads II, III and avF
Ectopic Atrial Tachycardia
- Rates are usually slower than AF ranging from 150-250 and can be irregular
- P-waves morphology differs from that of sinus P-waves as they are originating from an ectopic focus distal from the sinus node
- There is an isoelectric interval between P-waves in all leads
- When the rate is fast, the AV node will start to block signals
- In some cases, the P-waves can be small and dysmorphic, making them difficult to distinguish from the baseline
While it is important to see the distinction between atrial flutter and ectopic atrial tachycardia, the management of these patients is similar. The basic principles of management include AV nodal blockers and antiarrhythmic if the patient is stable and DC cardioversion if the patient is unstable. The definitive management is often ablation for these types of arrhythmias as they usually originate from a specific focus in the atria. This was the case in our patient, who underwent ablation at another institution.
nchristopher
Latest posts by nchristopher (see all)
- What’s wrong with this picture? – Answer - September 11, 2013
- What’s wrong with this picture? - August 21, 2013
- EKG Case 8 – Answer - July 16, 2013
- EKG Case 8 – All that wheezes - June 19, 2013
- EKG Case 7 Answer - June 19, 2013
1 comment for “Rhythm Nation: Case 1 Solution”