
ANSWER
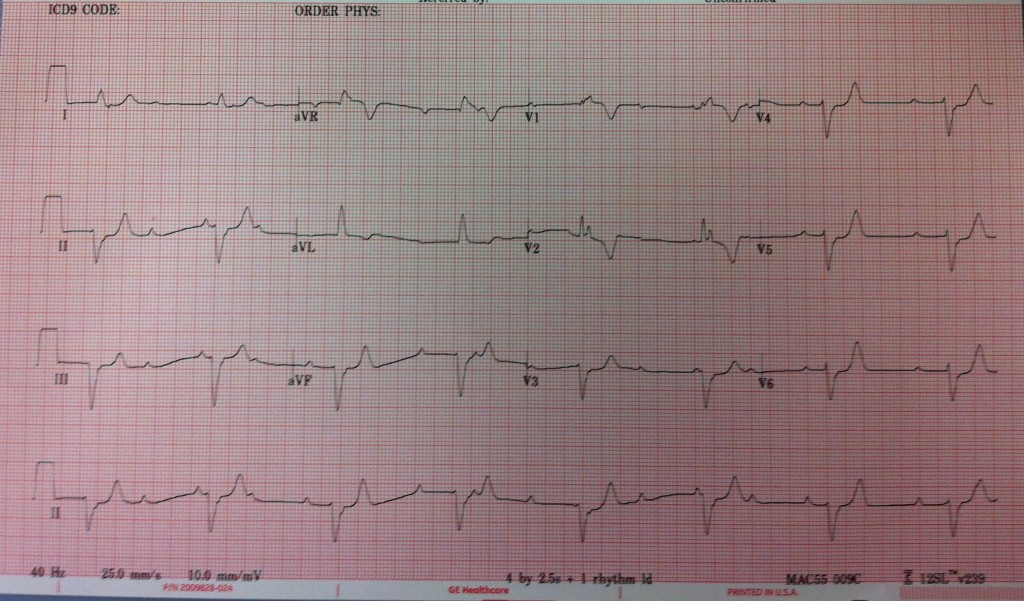
The first thing to note with this EKG is the 3rd degree heart block. As you can see, there is no clear associated between the P waves and the QRS. A good way to do this in practice is to mark the PP interval on the rhythm strip and march it out. In this EKG you can clearly see areas where the P falls directly on the QRS and other areas where there is no QRS between the P waves.
Next we look at the morphology of the P waves. Normal P wave axis is between 0 and +75 which means they should be upright in I and II and inverted in AVR. The normal P wave is monophasic in lead II and biphasic in V1. Atrial enlargement can be seen by a tall P wave in lead II (P-pulmonale). The enlarged right atrium takes longer to contract and thus, the right atrial depolarization which usually happens slightly before the left falls on top of left atrial depolarization causing the P wave to be tall. In left atrial enlargement a notched P wave is seen in V1 (P-mitrale). This is caused by the larger left atrium depolarizing slower and causing more separation between the right atrial and left atrial depolarization.
Next, we look at the rhythm strip to make sure the P wave morphology is consistent. In other words, every P wave in a single lead should look the same. P waves with changing morphology suggest an ectopic source of the P waves other than the SA node. In this EKG, we see that the morphology of the P waves is consistent, with a normal axis and no signs of atrial enlargement.
The other abnormality on this EKG is the ventricular rhythm. The QRS is wide and you see an RSR’ pattern in V1 and V2. However, you don’t see the typical wide slurred S wave in V6 to suggest RBBB. Also the QRS axis stays predominantly negative in the precordial leads. The overall QRS axis shows a left deviation. Furthermore, the qR pattern in I and AVL and the rS pattern in the inferior leads suggests a left anterior hemi-block. The ventricular rate in this EKG is 54 which is consistent with a junctional rhythm originating from the AV node.
Thus this EKG shows 3rd degree heart block with a left anterior fascicle block and an incomplete RBBB pattern. In this patient, these findings are secondary to systemic sclerosis and infiltration of the conduction system. This patient required an implantable pacemaker
mritchie
Latest posts by mritchie (see all)
- X-ray Vision: The answer - July 31, 2013
- X-ray Vision: Ortho - July 17, 2013
- X-ray Vision Answer: - April 17, 2013
- X-ray Vision: Stories in the chest x-ray - April 2, 2013
- Rhythm Nation: Case 6 Answer - March 23, 2013
2 comments for “Rhythm Nation EKG #3 – October – Answer!”