
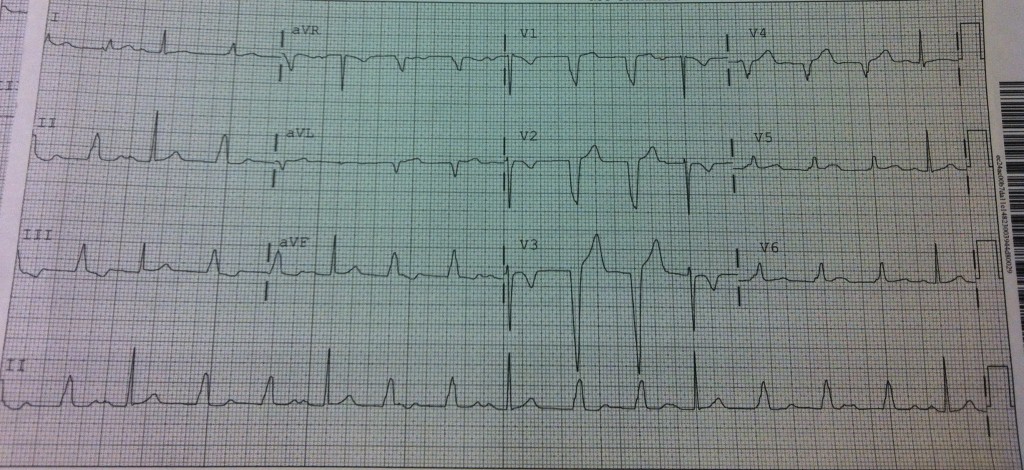
This 18yo F presented with one episode of chest pain which lasted a 2-3 minutes, was left sided, sharp and 8/10. Vitals in the ED were BP 112/71 HR 106, RR 18, T98.9. The above EKG was obtained as part of the workup for ACS.
Post your questions/comments or an interpretation in the comments and the answer will be posted next week!
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

nchristopher
Latest posts by nchristopher (see all)
- What’s wrong with this picture? – Answer - September 11, 2013
- What’s wrong with this picture? - August 21, 2013
- EKG Case 8 – Answer - July 16, 2013
- EKG Case 8 – All that wheezes - June 19, 2013
- EKG Case 7 Answer - June 19, 2013
6 comments for “Rhythm Nation: Case 5”