
Thanks Dr. Grock and Dr. Freedman for your responses. Sorry for the delay in posting the answer. Before we do get to the answer… a little more of the history:
Our patient was is an 18yo F who’s only past medical history if that of an arrhythmia 3 months ago in St Vincent’s. She is an avid soccer player and part of the national team at home and moved to the US to pursue a professional soccer career. She presented to the ED with chest pain that started 7am the day prior while the patient was standing for a few minutes. She was not doing any exertional activity around the time of the chest pain. She described the pain as left sided, localized near the shoulder, sharp, 8/10 lasting 2-3 minutes and resolving without any intervention. She had no associated dizziness, diaphoresis, nausea, vomiting, palpitations or shortness of breath.
Her previous episode of chest pain was in April 2012 in St Vincent’s where she was admitted to the ICU and told that she had a “fast rhythm and heart block”. She was seen by a cardiologist there and discharged on atenolol and isosorbide denigrate but she has not been compliant with these medications.
While we have no prior EKGs the patient had repeat EKGs shown below:
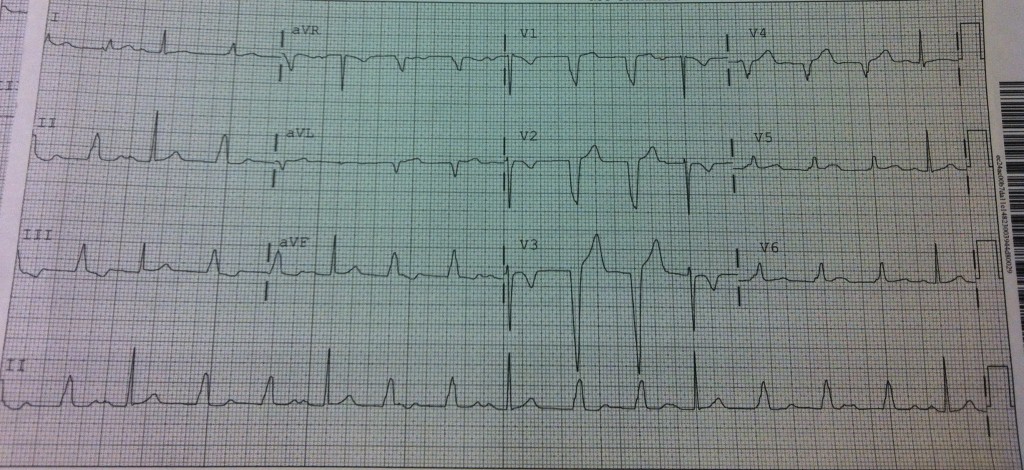
EKG1
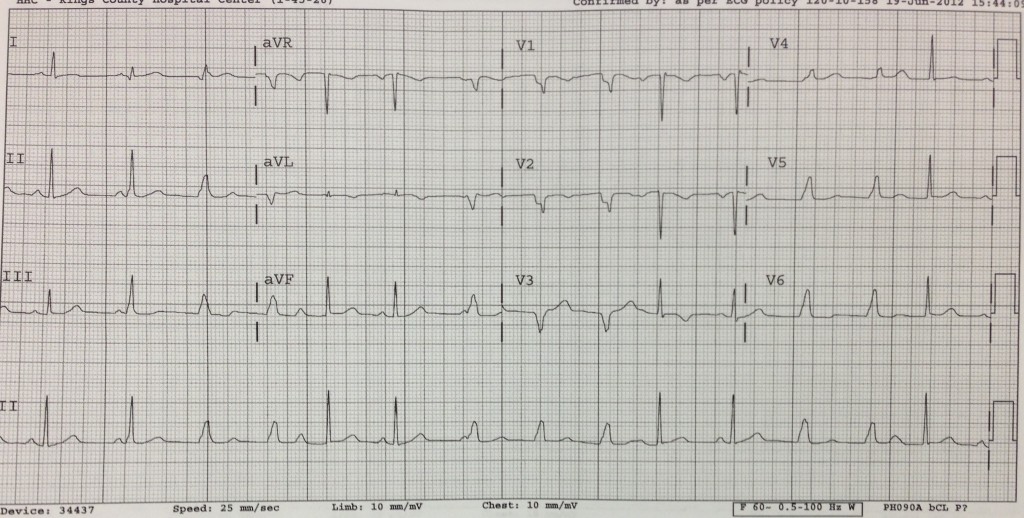
EKG 2
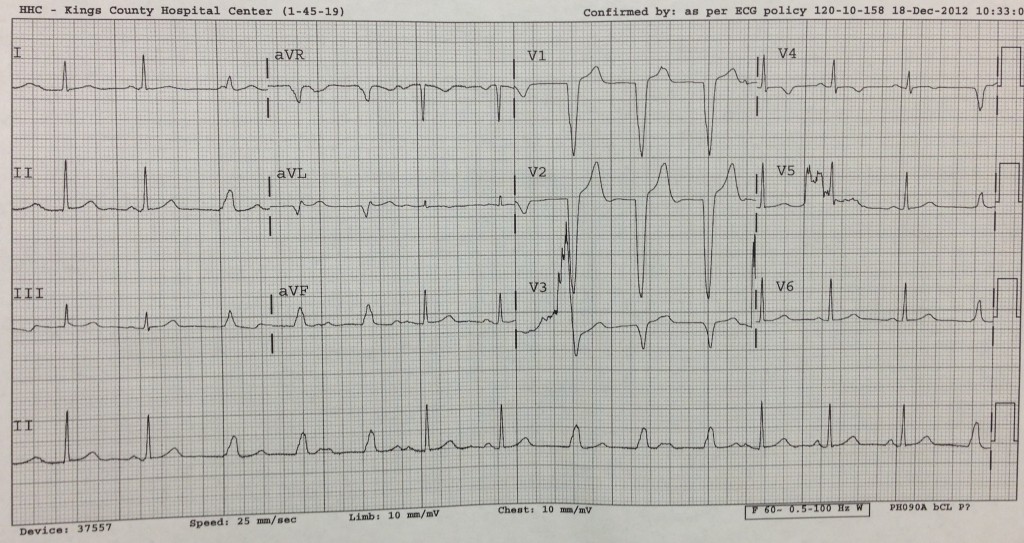
EKG 3
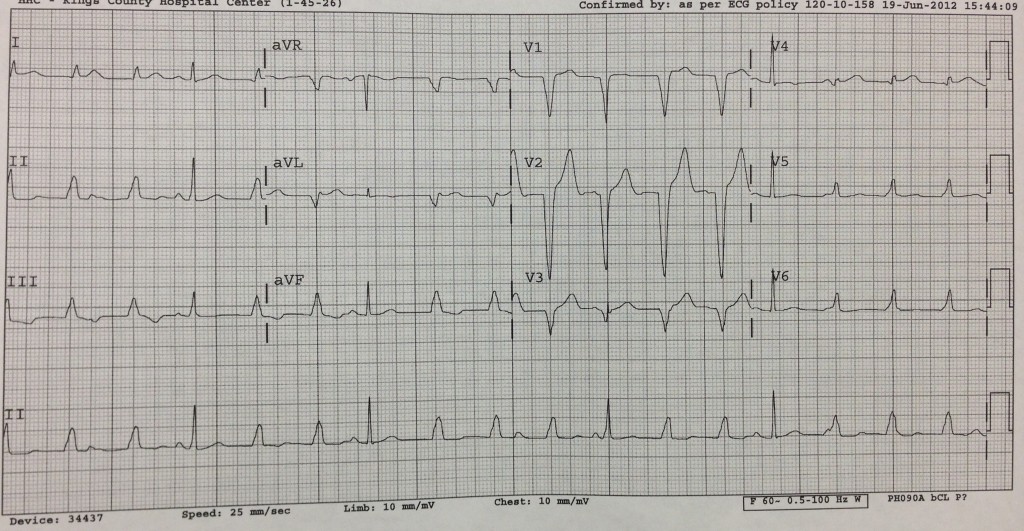
The first thing to note about these EKGs is that they all show 2 distinct morphologies of the QRS. In every EKG you see some QRS beats that are narrow and some that are wide. The narrow QRS complexes are almost always preceded by a P wave although the PR duration is variable, ranging from its narrowest at 160ms on EKG 3 to its longest on the original EKG at 280ms.
The wide complex QRS beats are also seen in every EKG and occur in couplets or triplets with a QRS duration of just over 120ms. These wide complex beats are not preceded by P waves. However, in nearly all the EKGs if you map out the P-P duration the first wide complex beat falls where the next sinus P wave should fall. In some cases (rhythm strip of EKG3 and EKG1) you can see a small deflection merging with the first wide complex beat which may be a buried P wave. In addition, the R-R interval between any of the wide complex beats in one EKG is always the same, suggesting these beats are originating consistently from the same place in the heart. Just looking at the wide complex beats, the pattern that emerges is a LBBB pattern with a dominant S wave in V1 and R wave in V5-6.
So, putting it all together we get:
Rate: If you map out the rate of the wide complex beats you get a rate of 88BPM (60/RR interval = 60/0.68 = 88). For the sinus beats the rate is variable, ranging from 75 to 88.
Rhythm: Alternating sinus beats with wide complex beats. Although we do occasionally see P waves within the wide complex beats we do not see them marching throughout the rhythm strip so this is unlikely to be complete heart block.
Axis: Up in I, aVF and II = Normal axis
Intervals: PR interval is not consistent, ranging from normal to 1st degree AV Block. In the EKGs where we do have consecutive sinus beats, the PR interval seems to be narrowing with each consecutive beat, rather than lengthening which means it is unlikely to be Wenckebach. Furthermore the fact that we do not see dropped beats (P waves without corresponding QRS complexes) argues against any type of 2nd degree AV block.
ST Segments: There is no evidence of ST elevations or depressions. The T waves associated with sinus beats do not show any significant inversions or flattening, however those associated with wide complex beats are often biphasic or inverted suggesting abnormal repolarization likely secondary to the abnormal conduction of these beats.
Chambers: No signs of left ventricular or atrial hypertrophy. No signs of right atrial enlargement.
Given the information above, the most likely diagnosis is an Accelerated Idioventricular Rhythm (AIVR).
Congratulations Dr. Freedman for the correct answer!
AIVR occurs when the rate of an ectopic ventricular pacemaker exceeds that of the sinus node. Normal ventricular pacing runs at 20-40 BPM while junctional escape rhythm runs at a rate of 40-60 BPM. AIVR can occur in cases of increased vagal tone and decreased sympathetic tone. Its mechanism is due to enhanced automaticity of the ventricular pacemaker, causing it to exceed the normal rate of 60 BPM which can be triggered by digoxin toxicity, electrolyte abnormalities, cardiomyopathy, myocarditis or ischemia. The EKG features include a rate of 60-110, regular rhythm, QRS complexes > 120ms and the presence of fusion/capture beats.
Our case highlights a specific cause of AIVR in young healthy patients – the Athletic heart. Athletic training leads to increased vagal tone and decreased sympathetic tone which suppresses both the SA and AV node resulting in sinus bradycardia and 1st degree AV block in some cases. When this is coupled with an idioventricular pacemaker, these pacemakers compete for capture. When the sinus rhythm rate goes above the idioventricular pacemaker’s rate, we see sinus capture beats.
If the sinus and ventricular pacemaker are running at similar rates, you can see Isorhythmic AV dissociation. This occurs because the retrograde ventricular impulses depolarize the AV node and make it refractory to the impulse coming from the SA node. In our EKGs this is evidenced by the fact that there are no P waves noted between wide complex beats. This helps to differentiate between 3rd degree heart block where the atrial rate is usually faster than the ventricular rate and P waves are seen marching through the QRS complexes.
In cases of AIVR, patients should not be given antiarrhythmics or beta-blockers as this can further slow the SA node and allow the idioventricular rhythm to dominate, which may lead to hemodynamic compromise. The underlying cause should be treated… electrolytes, dig toxicity, ischemia. Alternatively, if AIVR is suspected and the patient is symptomatic, atropine can be used to increase the sinus rate to overcome the idioventricular pacemaker. This restores AV synchronicity and allows to atrial kick to help improve cardiac output.
Conclusion:
Our patient was admitted to medicine and cardiology was consulted. They remarked that the rhythm could be an accelerated junctional* vs idioventricular rhythm having features of RVOT origin. She was transferred to Bellevue hospital for further workup and management. During her stay at Bellevue she was noted to have an accelerated idioventricular rhythm that was suppressed when she excercised. She had a cardiac MRI which showed an abnormality of the midlevel of the RV free wall – aneurysmal bulging, abnormal wall motion, abnormal enhancement – which could be consistent with Arrythmogenic Right Ventricular Cardiomyopathy (AVRC*). Pt had an electrophysiology study and which did not note any abnormality in the area indicated by MRI but localized an inducible ventricular tachycardia to the RV moderator band* which was ablated with resolution of symptoms and normalization of the EKG.
NOTES:
*Accelerated junctional rhythm is unlikely in our patient because of the presence of capture beats. (more info here)
*Arrhythmogenic Right Ventricular Cardiomyopathy – Usually presents with right ventricular outflow tract tachycardia which is a monomorphic VT with LBBB and inferior axis. When not in VT, these patients have some classic EKG findings including epsilon wave and prolonged S wave upstroke in V1-3. Unlikely in our patient who’s EKG had many capture beats and a rate that was too slow to be VT. (See here and here)
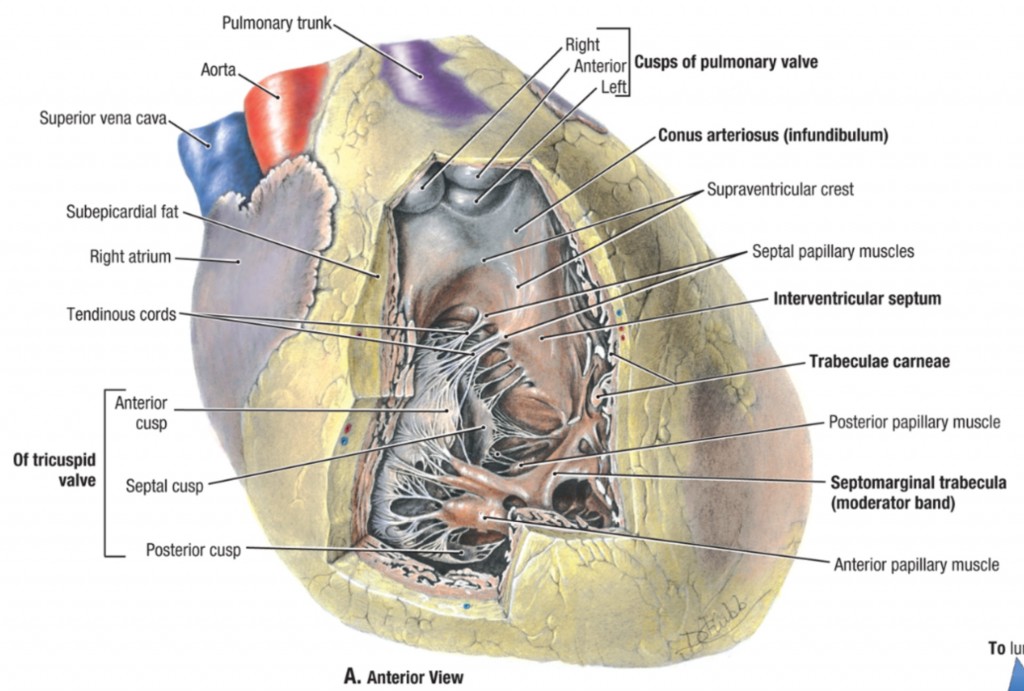
*RV moderator band – carries part of the R bundle branch to the anterior papillary muscle and RV free wall.
nchristopher
Latest posts by nchristopher (see all)
- What’s wrong with this picture? – Answer - September 11, 2013
- What’s wrong with this picture? - August 21, 2013
- EKG Case 8 – Answer - July 16, 2013
- EKG Case 8 – All that wheezes - June 19, 2013
- EKG Case 7 Answer - June 19, 2013