
Today’s Morning Report is courtesy of Dr. Basile!
Delayed Sequence Intubation
Why do this?
– Standard preoxygenation with NRB mask (65-80% FiO2) for 3 min or 8 vital capacity breaths has been shown to provide a buffer of 8 min in a healthy, non-obese adult patient before desats to the 90% threshold.
– To safely intubate the subset of critically ill patients (injured lungs, abnormal body habitus, or upregulated metabolism) where conventional preoxygenation techniques fail to provide adequate preoxygenation and therefore lead to desaturation
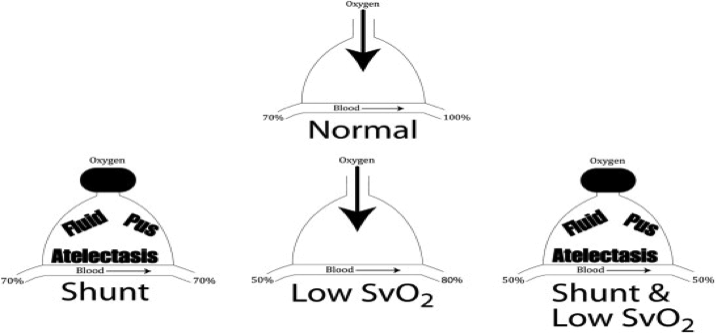
Quick pathophysiology of hypoxemia in the ED:
– Physiologic shunt is the major cause of poor oxygenation in sick ED patients on oxygen –> areas of alveoli are blocked from conducting oxygen, but still have intact blood vessels surrounding them leading to perfusion WITHOUT ventilation (Pneumonia, ARDS, Atelectasis, Pulmonary Edema, Mucous Pugging)
– Increasing FiO2 will not improve physiologic shunt
– In shock states, venous sat is lower than in healthy patients and require more oxygenation in order to increase venous sat to 100% (combined with shunt worsens problem)
Preoxygenation of Critically Ill Patients:
– A patient with sat <95% on nasal cannula at 6 L has at least some shunting
– A patient with sat <95% on NRB has moderate to severe shunting
– Don’t rush to intubate the patient who is satting < 90% on NRB
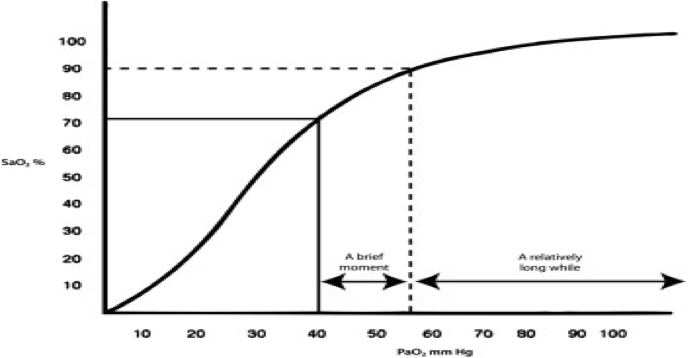
– RSI may cause an immediate and significant desaturation almost immediately after RSI drugs because the patient is already on the steep portion on the oxygen-hgb dissociation curve
– Amount of time for desaturation from 100% to 90% is much greater than from 90% to 80%
– Noninvasive Ventilation will give an FiO2 of 100% with a properly fitting mask (at CPAP of 0) and with increased CPAP settings, shunt can actually be treated and improve patient’s oxygenation
Delayed Sequence Intubation:
– Hypoxic and hypercapnic patients can become agitated/delirious causing them to rip off NRB/NIV masks and become noncompliant
– There is another alternative to rushing to intubate these patients via RSI
– DSI consists of administering specific sedative agent (ketamine) that does not blunt spontaneous ventilations or airway reflexes followed by a brief period of preoxygenation before administration of the paralytic
– DSI is procedural sedation where the procedure is effective preoxygenation
– The dissociative state allows the application of NRB/NIV mask in a safe controlled fashion in a calmed patient
– 1-1.5 mg/kg ketamine by slow IVP
– allow the patient to increase sat to 100%
– allow the patient to breathe the high FiO2 for another 2-3 min to preoxygenate prior to paralyzing and intubating
Summary:
– Be aware of physiologic shunting and low venous sat in critically ill shock patients
– Be aware of oxygen hemoglobin dissociation curve
– Importance of preoxygenation and consider DSI
References:
S.D. Weingart. Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. J Emerg Med, 40 (2011), pp. 661–667.
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015