
Thanks to Dr. Desmond for today’s Morning Report!
Pediatric Thoracic Trauma
Thoracic trauma in children is relatively uncommon. Usually from high force injuries such as falls or motor vehicle accidents (75%) and is usually blunt.
When in isolation, mortality rate is low, however it TRIPLES when accompanied by head or abdominal injury.
Most common injuries are: 53% lung contusions, 38% hemo/pneumothorax, fractures 38% in blunt trauma.
Penetrating: 64% with hemo/pneumo, 15% diaphragm, 13% cardiac, 10% vascular.
Mortality: 10% in isolated rib fractures, 20% in blunt hemo/pneumo, up to 50% if heart involved.
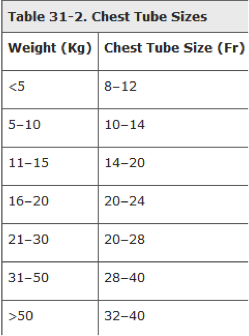
Evaluation of hemothorax: chest tube side is approximately the “size of the intercostal space” That is 16-24F.
Each hemothorax can hold 40% of a child’s blood volume, enough blood loss to lead to decompensated hemorrhagic shock.
Massive hemothorax: initial evacuated volume exceeding 10 to 15 mL/kg of blood or continued blood loss exceeding 2 to 4 mL/kg/h. Continued air leakage may be another reason to go to surgery.
Bronchial Tree Injury: Rather than collapsing toward the hilum, the lung seems to have fallen to the dependent portion of the thorax. This is called the “fallen-lung sign.” This is an extremely rare finding on x-ray, but when present, the abnormal position of the lung, together with the left-sided pneumothorax, are highly suggestive of rupture of the tracheobronchial tree.
Sources: AccessPediatrics, Pediatric Emergency Medicine, Textbook of Pediatric Emergency Medicine
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015