
We like to think we’re always practicing evidence-based medicine. So we inform our consultants about likelihood ratios and ask how can they be “so sure.” We try to be very aware of the sensitivities and specificities of the tests we use so that their results can be qualified. But sometimes, we forget that all information comes to us via one kind of test or another. Tests and the answers they give us are often not gold standards that we believe them to be. Pulse oximetry is no exception. And yet, we’re obsessed with it. We bank on it. We are reassured by it. And it’s easy to understand why. The airway and breathing processes are fundamental and complicated. Pulse-oximetry gives us an easy answer, a fast number. And we love numbers.
Ok. To say that one hates pulse-ox is clearly an overstatement. Got a beautiful waveform with a scary number? That’s solid info, especially in a patient in whom you suspect an A-a gradient, ie. pneumonia, CHF, ARDS, PE, sepsis. No question, hypoxemia is important. It’s one of the original “H and T” killer bees. We care about oxygenation. So we use and then overuse pulse-oximetry. In doing so, it’s easy to forget what pulse-ox is and isn’t. Pulse-ox is an amazingly useful method for determining arterial hemoglobin saturation in the distal arterioles of your finger. It is not real-time, central oxygen saturations in the places we care about, ie. brain and heart. Unfortunately for us, ED docs, who deal in acute airway management, pulse-oximetry does a poor job standing in for the gold standard. Here’s why.
Pulse oximetry is a time-machine
With pulse-oximetry, we are looking into the past. In healthy people with decent cardiac output, pulse-ox shows where central saturations were 30 seconds ago.[i] For those sick, with poor cardiac output or in a shock state, ie. those requiring RSI, you’re looking even further into the past, 90 seconds or longer.[ii] 90 seconds! We know this exists. Why else would we use color-metrics to confirm ET tube placement? In a series of esophageal intubations, pulse-oximetry was unable to detect incorrect tube placement for thirty seconds.[iii] Forget about those sick enough to not even register a waveform. Anesthesia data predict that the patients most likely to have pulse-oximtery failure are those with hypotension and/or hypothermia.[iv] Hello, RSI.
One of the hallmarks of managing the acutely failing airway is avoiding hypoxemia. And we care deeply what a patient’s saturations are. It’s just that pulse-oximetry can’t accurately tell us how we’re doing acutely. So how do we know we’re getting good oxygenation? Well…It’s as simple as moving air. Check this old-timey physiology graph?. It’s the alveolar-gas equation mapped out at different Fi02s.
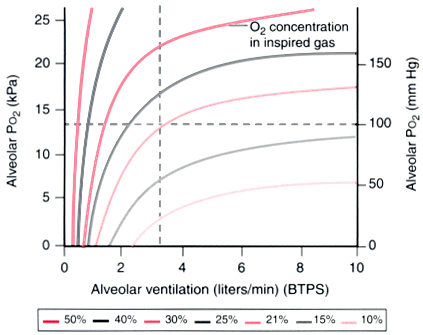
What jumps at me is how little bits of minute ventilation with high Fi02s generate fantastic alveolar oxygen pressures. Let’s put it to a case: at only 40% FiO2, (which is totally plausible during resuscitation) it takes only 1L/minute of air-moved to achieve an alveolar P02 of 100mmHg. Think about that. 1L/min! It’s mind-boggling. That’s only two tidal volume breaths a minute!
So you’re saying, “Wait a sec. Something’s off. I deliver 10x that much air during assisted ventilation!” And you’d be right. The above-relationship is between alveolar ventilation and oxygenation. Alveolar oxygenation does not equal arterial oxygenation. Oxygen has to move from the alveolar space into the blood: the A-a gradient. To overcome shunt or V/Q mismatch in acute airway management, we have limited tools. We can control the airway and move a volume of high-FiO2 into the alveoli. We can increase PEEP (think PEEP valves for BVM). That’s about all we got. Just move air. And how do we know we’re moving air? Certainly not pulse-ox. (We’ll save capnography for another time.)
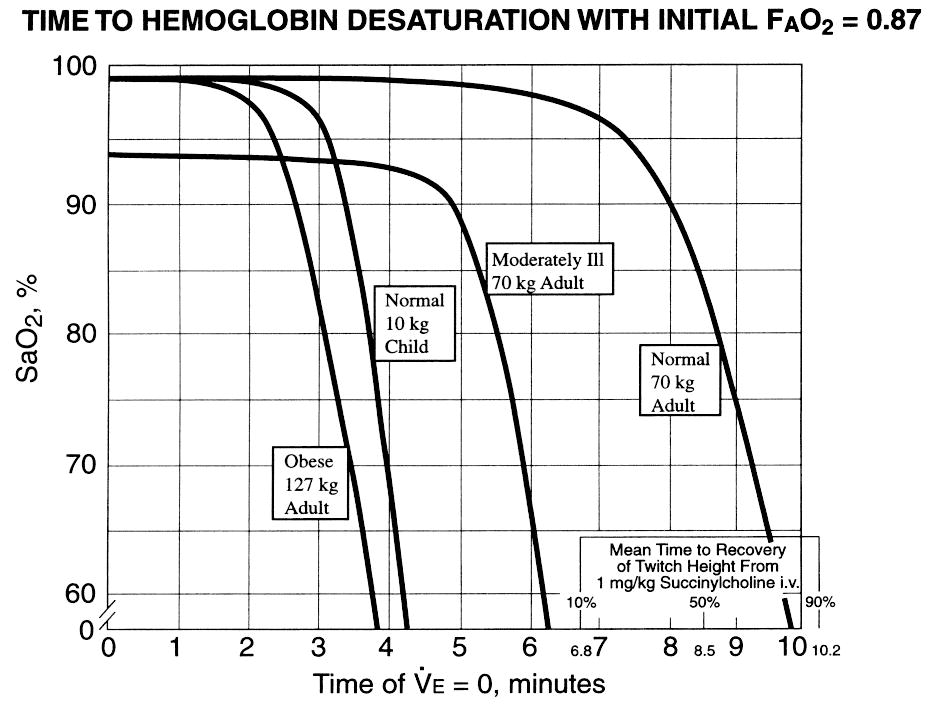
So just how bad is pulse-oximetry at determining air movement? We know from “apneic oxygenation” that it takes time to desaturate.[v] We know pre-oxygenation with high Fi02 extends the safe apnea time dramatically.[vi] Indeed, our bodies have evolved a miraculous safety system to continue oxygen delivery in moments of stress/apnea/hypoventiliation. For a healthy adult, breathing 90% FiO2, we’re talking 8 minutes of apnea time prior to an O2 sat of 90%. 8 minutes before central oxygenation gets critical! In acute airway management, the utility of staring at the pulse-ox for a pre-oxygenated patient approaches meaninglessness.
Ever wonder why ENT asks over the phone for the pulse-ox reading on your stridorous patient? If the upper-airway patient had been hypoventilating for long enough to produce pulse-ox changes, then the consultant would be hearing about a cricothyrotomy instead of a scope/
The inability of pulse-oximetry to detect early hypoventilation is compounded by its time lag. And yet, it is so often used as such. How often do we find everyone during an airway code staring at the pulse-oximeter, even reading off changes in the pulse-ox? How often (outside the ED) is pulse-oximetry the respiratory monitor for conscious sedation?
We often speak judgmentally about numbers and about “treating” them. But every day, we’re all guilty of the same fundamentally flawed thinking. We conflate the results, numbers, and images that we’re given with the gold standard. Often we make a logical leap of faith, saying that these results are surrogates for the truth. But, they’re not. And we know it. Maybe they’ve got something to do with the truth and can shed some light. But they’re just tests, flawed by their own properties. The more that we rely on them without understanding them; the more we’ll be unable to separate the answer they give from the truth we seek. True from auscultating lungs, to serum sodium, to CT scans, to stress tests, to you name it. To pulse oximetry.
I know that we’re all not guilty all the time. But the propensity exists to put too much stock in a number. Use judgment and understand the tools at your disposal. In so doing, we’ll be stronger clinicians.
Take-away points: 1. Pulse-0x lag is real and limits the utility of pulse-oximetry for acute airway interventions. Always confirm air movement via other means that pulse-ox. And 2. If you’re ruling out hypoventilation and the pulse-ox has already fallen, you’re way late.
Tobias JD. Cerebral oximetry monitoring with near infrared spectroscopy detects alterations in oxygenation before pulse oximetry. J Intensive Care Med.
2008;23(6):384-388
Xue FS, Liao X, Tong SY, et al. Effect of epidural block on the lag time of pulse oximeter response. Anaesthesia. 1996;51(12):1102-1105.
Reich DL, Timcenko A, Bodian CA, et al. Predictors of pulse oximetry data failure. Anesthesiology. 1996;84(4):859-864.
Guggenberger H, Lenz G, Federle R. Early detection of inadvertent oesophageal intubation: pulse oximetry vs. capnography. Acta Anaesthesiol Scand. 1989;33(2):112-115.
Weingart SD. Preoxygenation, Reoxygenation, and Delayed Sequence Intubation in the Emergency Department. J Emerg Med. 2010 Apr 7.
Heller ML, Watson TR Jr. Polarographic study of arterial oxygenation during apnea in man. N Engl J Med. 1961;264:326-330
Lumb AB. Nunn’s Applied Respiratory Physiology. 7th ed. Oxford:
Churchill Livingstone; 2010:568.
[i] Tobias et al, 2008
[ii] Xue et al, 1996
[iii] Guggenberger et al, 1989
[iv] Reich et al, 1996
[v] Weingart 2010
[vi] Heller et al., 1961
[vii] Lumb, 2010
jfreedman
Latest posts by jfreedman (see all)
- Less is More - April 13, 2015
- Don’t just do something, stand there. - January 19, 2015
- All pressure is created equal - September 15, 2014
- The “Soft” Code - June 23, 2014
- 6/25 Adult Journal Club - June 16, 2014
1 comment for “Hating on pulse-ox”