
Here’s Dr. Alsup with today’s Morning Report!
Wolf Parkinson White Syndrome
- Pre-excitation syndrome. Accessory electrical conduction pathway
 between atria and ventricle (most common tract name is “Bundle of Kent”)
between atria and ventricle (most common tract name is “Bundle of Kent”) - The incidence of WPW is between 0.1% and 0.3% in the general population
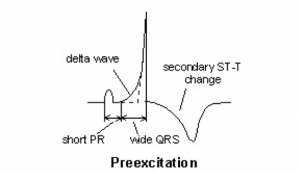
ECG Findings
• Normal P waves
• Shortened PR interval (75%)
• Prolonged QRS interval
• Delta waves (slurring of the initial upstroke of R wave)
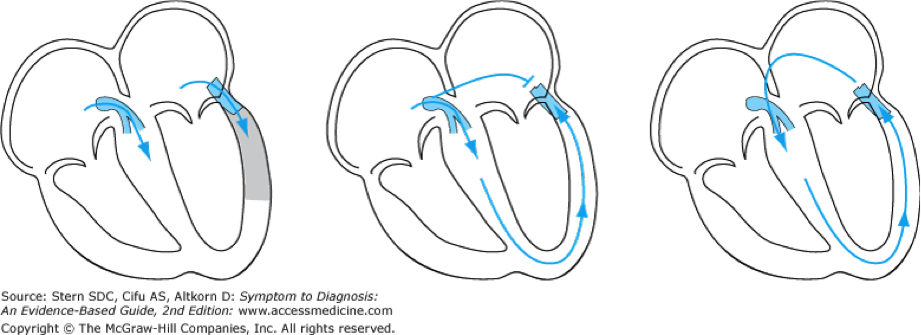
Associated tachydysrhythmias:
Orthodromic AVRT (antegrade conduction through the AV node, retrograde through accessory tract) accounts for 70–80% of arrhythmias in patients with AV bypass tracts, with heart rates of 140–250 bpm.
– Adenosine, calcium channel blockers, beta-adrenergic blockers, and procainamide are all suitable for first-line therapy if vagal maneuvers fail
– Patients with chest pain, congestive heart failure, electrolyte imbalance, other medical issues need admission.
Antidromic AVRT: reverse cyclical conduction (from atria, through accessory pathway, retrograde through AV node) is more rare, with a regular wide complex.
– This looks very much like Ventricular Tachycardia, but has regular P waves.
– It is difficult to differentiate this from afib with WPW, so it is treated as afib with WPW
Atrial fibrillation accounts for only 19–38% of arrhythmias in the population with accessory pathways, but it is potentially more lethal than the reciprocating tachycardias. It is more common in patients with antegrade conducting accessory pathways and in pathways with a short antegrade refractory period. By virtue of their short refractory periods, bypass tracts (unlike the AV node) have the potential to conduct very rapidly to the ventricles at ventricular rates of 250–350 bpm with the possibility of causing degeneration to ventricular fibrillation.
- Do not treat this tachycardia with AV nodal blocking agents (calcium channel blockers, b-blockers, digoxin, and importantly adenosine). This may lead to unopposed ventricular stimulation through the accessory tract and may worsen the tachycardia.
- Procainamide, amiodarone are accepted methods for conversion of tachycardia associated with WPW.
- Cardioversion for unstable patients (50-100J for adults and 0.5-2 J/kg for children)
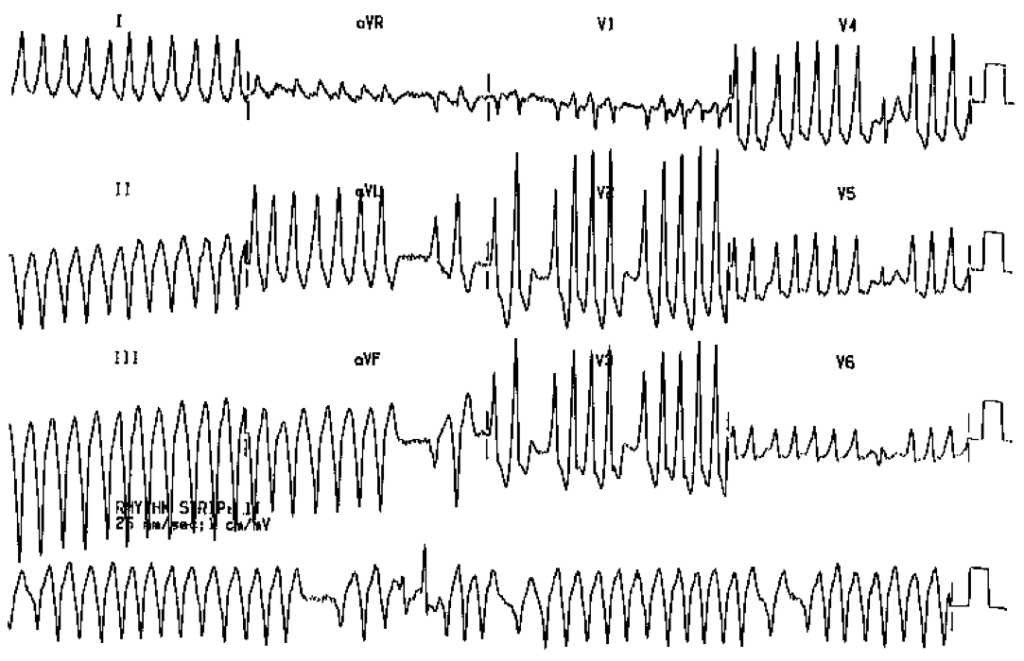
Example of Afib with WPW— very dangerous rhythm
References:
http://lifeinthefastlane.com/ecg-library/pre-excitation-syndromes/
Tintinalli’s Emergency Medicine
Hurst’s The heart
Rosen’s
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015