
Here’s Dr. Bon with today’s Morning Report!
Heat Induced Illness
Epidemiology:
1979-1999 – totally of 8,015 related deaths according to CDC
Heat wave – 3 or more consecutive days with air temps > 90
Heat related death – exposure to hot weather, body temp > 105, and lack of other cause of hyperthermia
Mechanism of heat damage:
1) Denaturation of proteins causing cellular dysfunction and leading to cell damage and apoptosis. Esp in thymus, spleen, lymph nodes and mucosa of small intestine
2) Induction of release of several inflammatory cytokines
3) Significant temp damage endothelium of vasculature and induce coagulation cascade resulting in DIC
Syndromes:
Heat Edema – benign condition, mild edema in dependent regions secondary to heat stress
Heat Tetany – carpopedal spasms caused from hypoventilation induced by heat stress
Heat Syncope – orthostatic hypotensive event secondary to peripheral vasodilation in response to heat stress, usually provoked by prolonged or sudden standing, tx – rest, cool environment, rehydration
Heat Cramps – sudden painful spasms in large voluntary muscle groups after prolonged exertion, thought to be due to large amount of sweat being replaced by hypotonic solutions. Tx –oral hydration with electrolyte containing solutions
Heat Exhaustion – profuse sweating , malaise, fatigue, nausea and possible vomiting. Tachycardia and often orthostatic hypotension. Temp < 104 and intact mental status. Tx – removal from heat and rehydration with electrolyte solution PO or IV depending on severity. Care should be taken to gradually replace significant free water deficits because of risk of cerebral edema
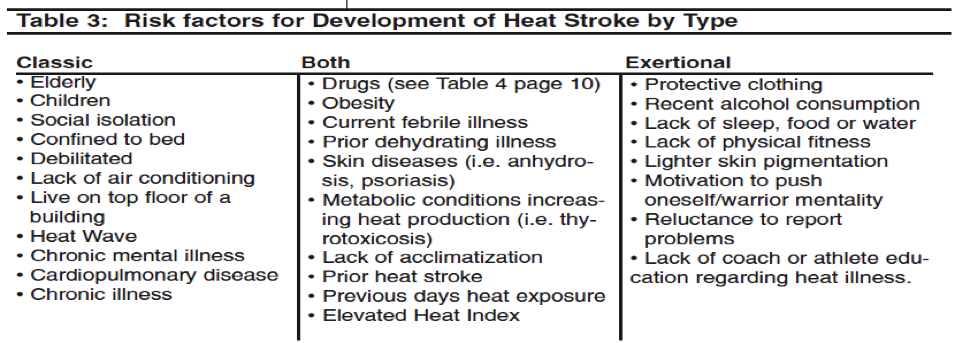
Heat Stroke – 1) a core body temp > 105 (though may be less) 2) CNS dysfunction 3) exposure to heat stress 4) exclusions sepsis, cns infection, NMS, malignant hyperthermia
- Two types: classic (epidemic) vs exertional
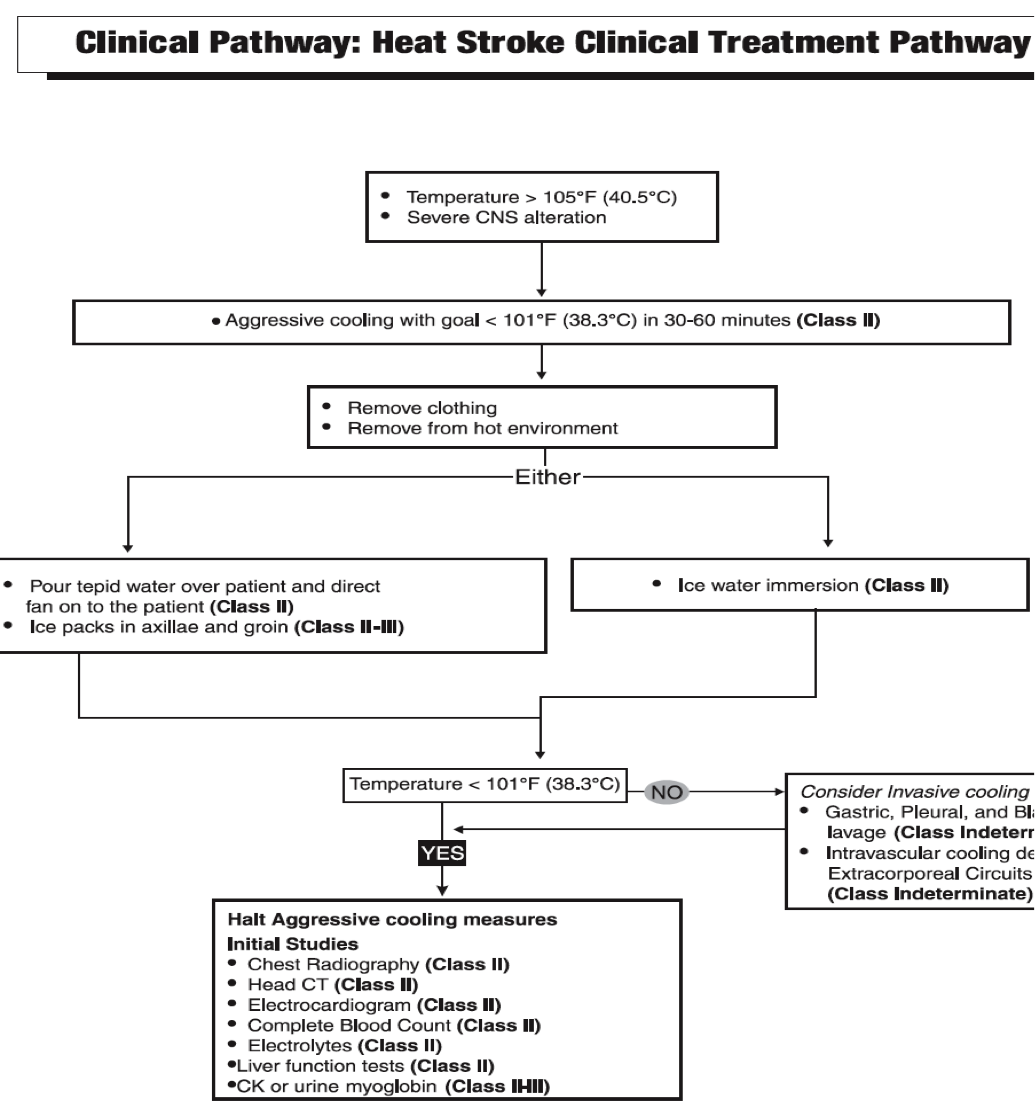
Management of Heat Stroke:
Initial – cardiac and pulse ox monitoring, core body temp measuring asap, foley catheter to measure urine output, consider CVC for monitoring of CVP
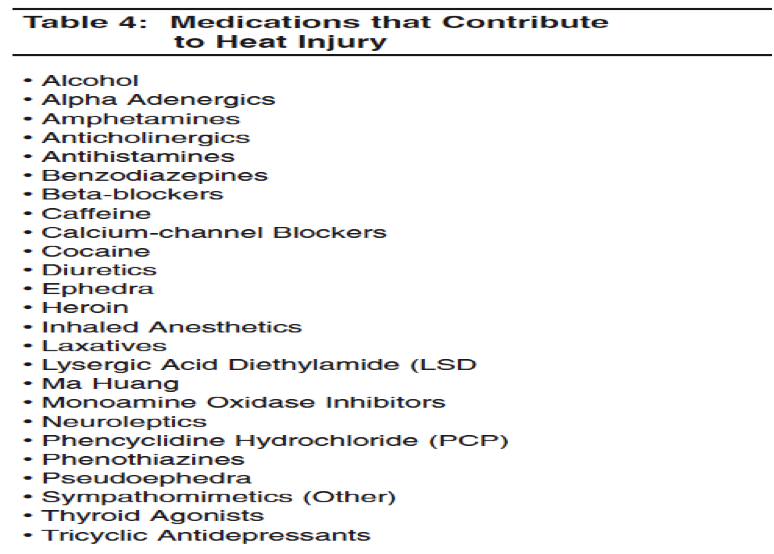
History – good history from EMS and witness to gauge timeline and context, predisposing medications, comorbidities
Physical Exam – ABCs – intubation may be required for airway protection depending on degree of ams, venous access and fluid resuscitation, hypotension is a concerning sign
Secondary PE: mental status/neuro – will gauge severity, includes speech, ataxia, confusion, coma, seizure, less common extrapyramidal syndromes
- Skin – sweating vs anhydrosis, turgor, bruising, petechaie (DIC)
- Lungs – access for pulmonary edema as additional cause of tachypnea
Studies:
- CXR (edema, ARDS)
- EKG– signs of ischema, afib, svt, most common QT prolongation
- CTH – reasonable if significant AMS (esp if DIC present)
- Labs – to access organ dysfunction ie hepatic, renal, rhabdo, DIC, electrolyte abnml
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015