
Today’s Morning Report is courtesy of Dr. Reisman!
This morning report we are reviewing a paper from a cardiology journal that proposes modification of the criteria for emergent cath lab activation. The goal is to recognize ECG patterns associated with acute coronary artery occlusion that do not present as a classic STEMI.
In addition, the authors recommend removing new LBBB as a criterion for cath lab activation, as this results in many negative caths.
There are 3 ECG patterns that represent acute coronary artery occlusion and do not have classic ST elevation. The authors do mention Wellen’s syndrome, but note that this pattern is typically associated with chronic rather than acute LAD disease, and requires non-emergent cath.
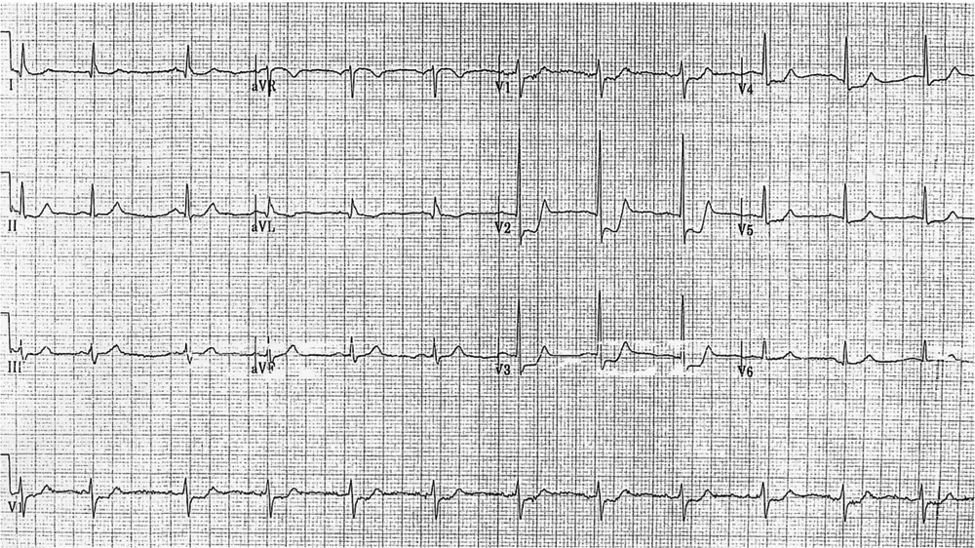
1) Posterior wall MI:
This ECG shows ST depression in leads V1-V3 without any ST elevation. This pattern is associated with acute occlusion of the left cirumflex artery. A posterior ECG can be performed to look for ST elevation.
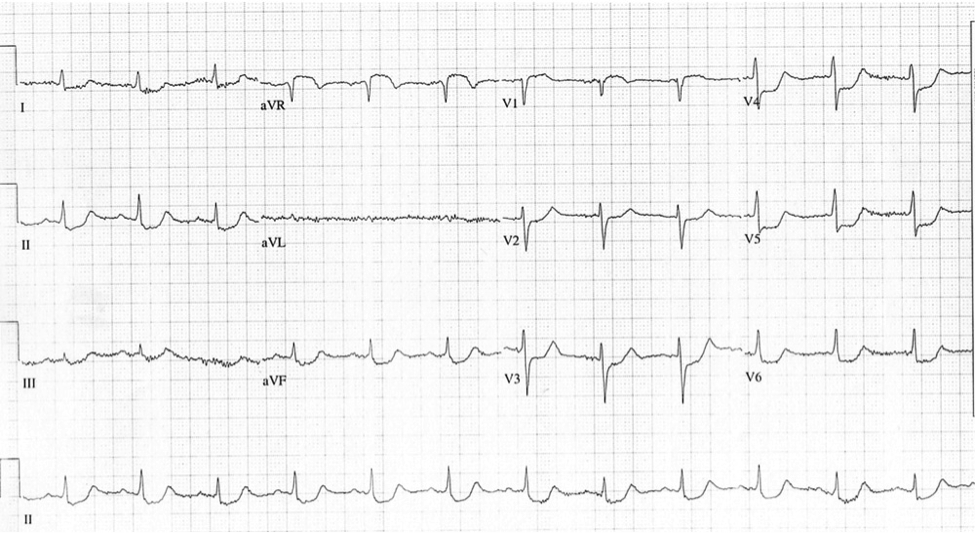
2) Acute left main coronary occlusion:
This ECG shows ST elevation in lead aVR greater than lead V1, with associated diffuse ST depression in multiple leads. This pattern is strongly associated with acute occlusion of the left main coronary artery. As the left main supplies both the LAD and the circumflex, most patients with left main coronary occlusion do not survive to the hospital. Of those that do survive to the hospital, mortality is greater than 50%. Of note, ST elevation higher in V1 than in aVR suggest occlusion of the LAD rather than the left main.
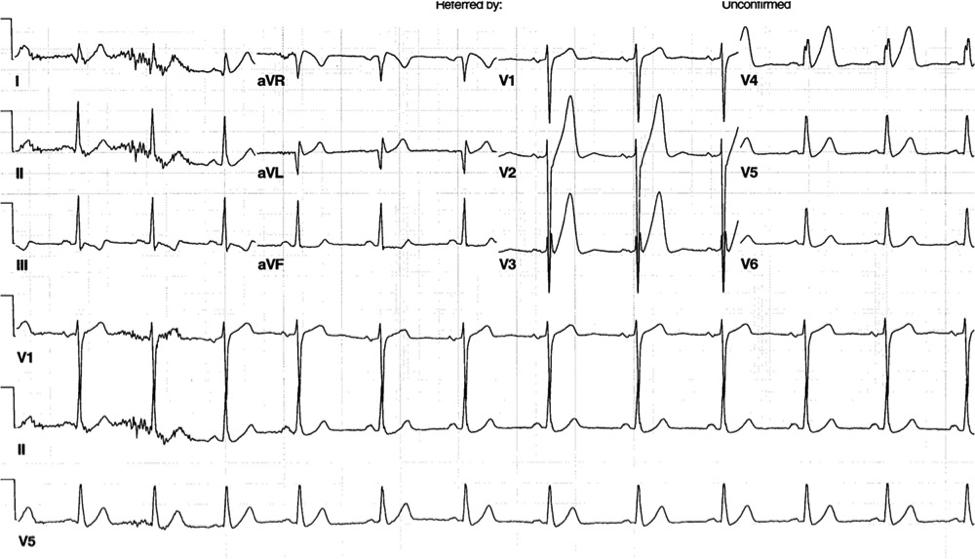
3) de Winter T wave pattern:
The de Winter T wave is a pattern consisting of ST depression of 1-3mm with upsloping at the J point and is associated with persistent tall symmetric t-waves in the precordial leads. In patient with normal potassium, this pattern is strongly associated acute MI. In the ECG below, the pattern is most obvious in leads V2 and V3.
Reference: Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. Rokos IC, French WJ, Mattu A, Nichol G, Farkouh ME, Reiffel J, Stone GW. Am Heart J. 2010 Dec;160(6):995-1003, 1003.e1-8. doi: 10.1016/j.ahj.2010.08.011.
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015