
Here’s Dr. Youn with today’s Morning Report!
Hyponatremia
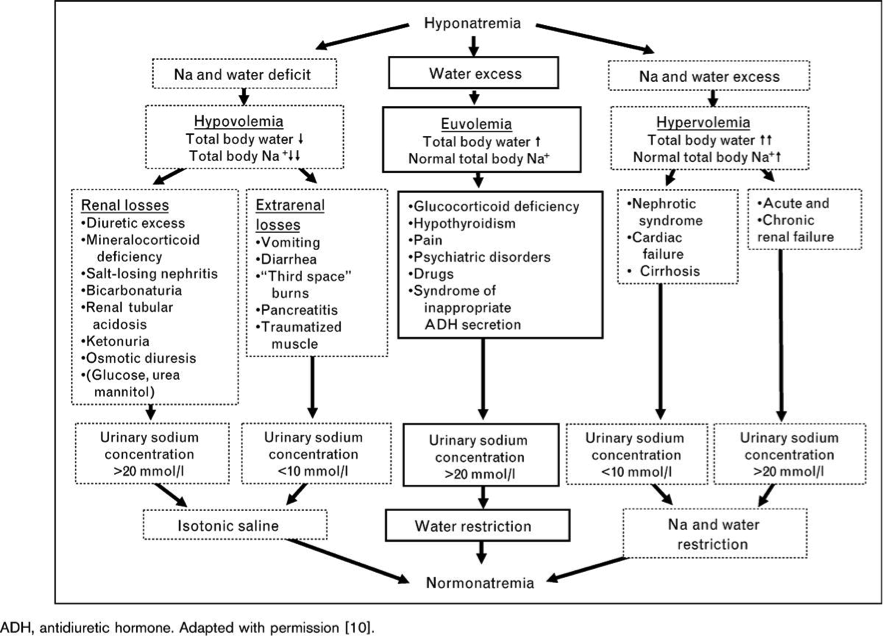
Source: Schrier RW and Bansal S. Diagnosis and management of hyponatremia in acute illness. Current Opinion in Critical Care 2008, 14:627-634
SERIOUS COMPLICATIONS: Cerebral edema, seizures, AMS, coma, death, iatrogenic (overcorrection of sodium)
INITIAL MANAGEMENT:
- ABCs, IV, O2, Monitor, H&P
- Labs:
- Serum: electrolytes, osmolality, uric acid (if on diuretics), TSH, cortisol
- Urine: UA, lytes, osm, urea, creatinine, uric acid (place foley)
- Treat symptoms (seizures, coma, herniation)
- 3% hypertonic saline – 100mL over 10-20 minutes (or over 1 hr or 4-6ml/kg/hr), repeat x1 if necessary (100mL will raise Na approx. 2mmol/L)
- Fluid restriction for euvolemic/hypervolemic; Isotonic hydration if clearly hypovolemic
- Rule of 6’s: only increase up to 6mEq/L per day. If patient has severe signs and symptoms, increase up to 6mEq/L within the first 6 hours and then stop.
- Consider dDAVP and/or D5W if concern for overcorrection; V2 vasopressin receptor antagonists – conivaptan, tolvaptan
- Osmotic Demyelination Syndrome – symptoms include dysarthria, dysphagia, seizure, AMS, quadriplegia, hypotension
- Be mindful of repleting potassium – if you replete K, then Na will increase as well
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.




Jay Khadpe MD
Editor in Chief of "The Original Kings of County"
Assistant Professor of Emergency Medicine
Assistant Residency Director
SUNY Downstate / Kings County Hospital
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015