
Here’s Dr. Youn with today’s Morning Report!
Lateral Canthotomy/Cantholysis
Emergent concern: retinal ischemia, optic nerve compression
Indications: Acute orbital compartment syndrome – usually 2/2 traumatic retrobulbar hemorrhage
Decreased visual acuity
IOP > 40 mmHg (normal range: 10-20)
Proptosis
APD
Contraindication: Globe rupture (teardrop pupil, positive Seidel test, enophthalmos, visible globe laceration, visible FB in eye)
Procedure:
- Stat ophthalmology consult
- Irrigate area with saline or sterile water – avoid betadine in eye
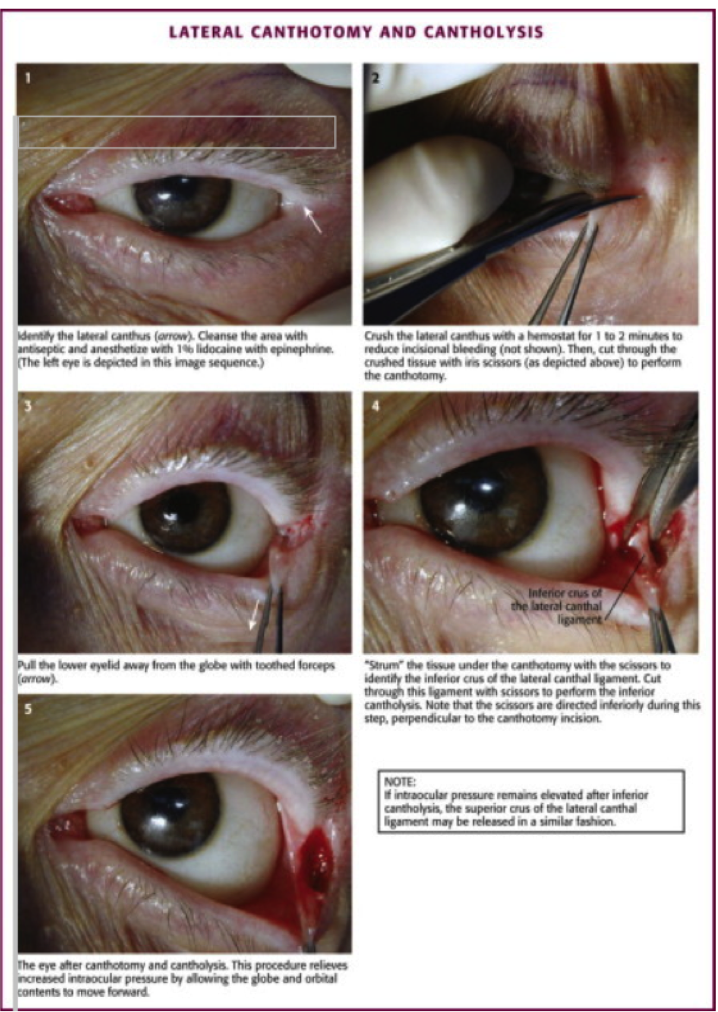
- Local anesthetic to lateral canthus – 1cc of 1-2% lidocaine with epi
- Apply hemostat to lateral canthus for 1-2 min to crush structures and decrease bleeding
- Cut laterally from lateral canthus to orbital rim – approx. 1cm
- Use forceps to retract lower lid down infero-laterally to expose inferior crus of lateral canthal ligament
- Cut inferior crus full thickness to orbital rim – lower eyelid should hang loosely
- Recheck IOP
- If still elevated, consider releasing superior crus of lateral canthal ligament.
- Discuss further medical management with ophtho if IOP still elevated – acetazolamide, topical beta blockers, mannitol, elevate HOB
- Definitive – ophthalmologic decompression
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.




Jay Khadpe MD
Editor in Chief of "The Original Kings of County"
Assistant Professor of Emergency Medicine
Assistant Residency Director
SUNY Downstate / Kings County Hospital
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015