
So for this post… we’re going to combine some EKG action with some good ole’ CXR reading… Since we’re not just doing Rhythm Nation or X-ray Vision… we’re going to call it Rhythm Vision!
Here’s the case:
Your patient is little old granny, an 85 year old woman with a history of CHF who normally goes to another institution for her care. She has a cardiologist there… but when you ask why she didn’t go to see her own doctor she says “I don’t like my cardiologist anymore, she keeps giving me the same meds over and over”. Her chief complaint is SOB and she states that she has been having progressive worsening of her shortness of breath and dyspnea on exertion. She also says her legs have been swelling up. She has no fever, chills, cough, chest pain, nausea, vomiting. She had no recent travel. She has never had a DVT. She says she’s taking all her meds, which include a water pill and the typical CHF meds (ASA, statin, B-blocker, ACE). She’s not on digoxin. Her exam reveals JVD, bibasilar rales and 2+ pitting edema to the knee. There is no calf asymmetry. You do a basic set of labs including cardiac markers and a BNP. The troponin is negative and the BNP is 900. Labs are otherwise unremarkable. You get the following EKG and CXR (click for larger versions)!
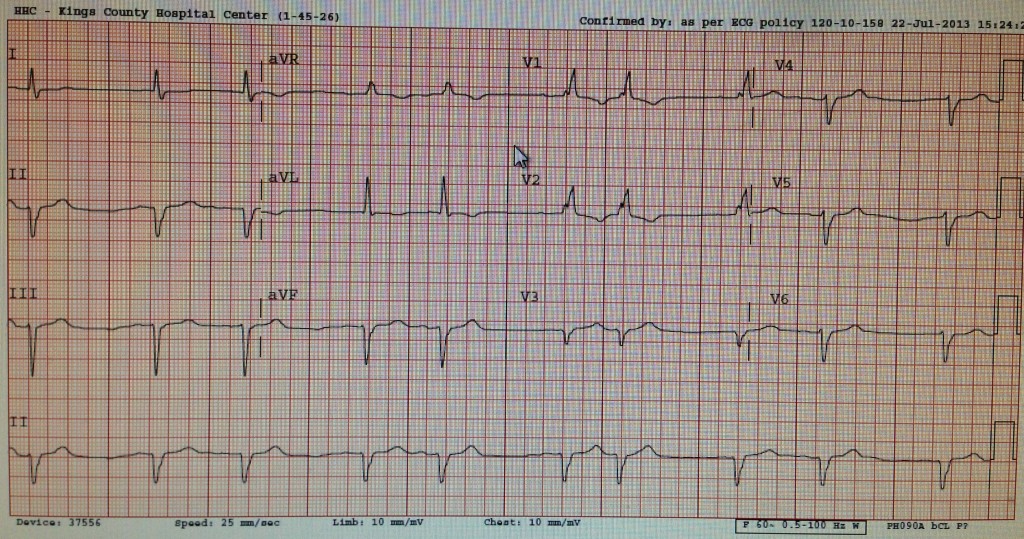
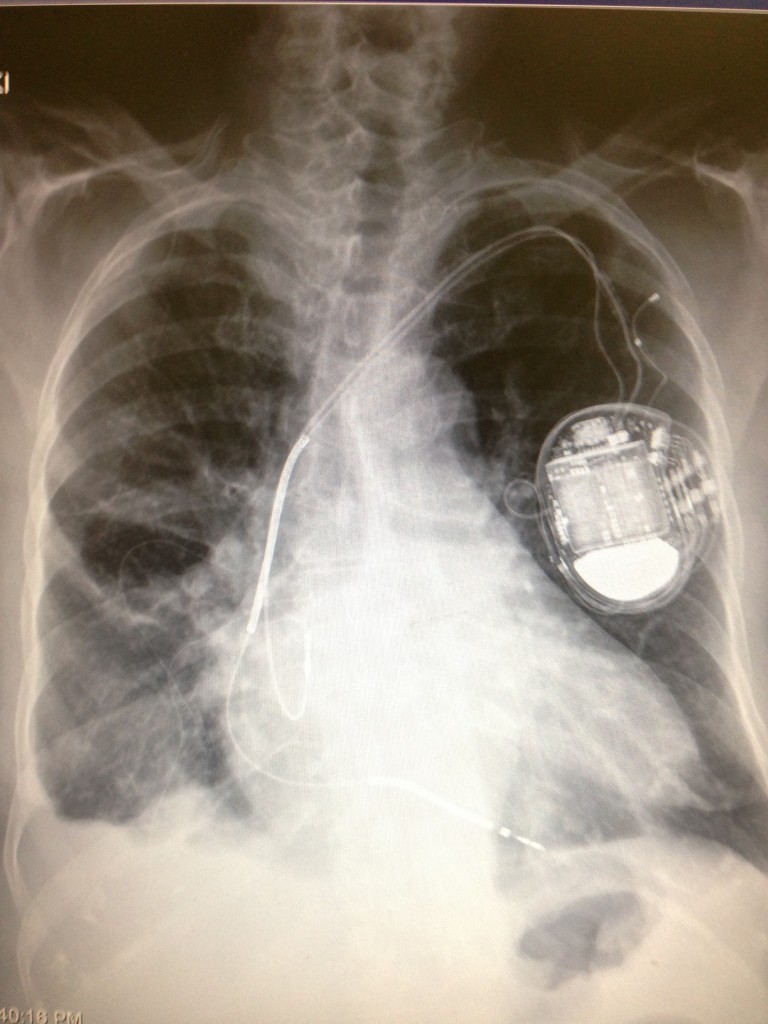
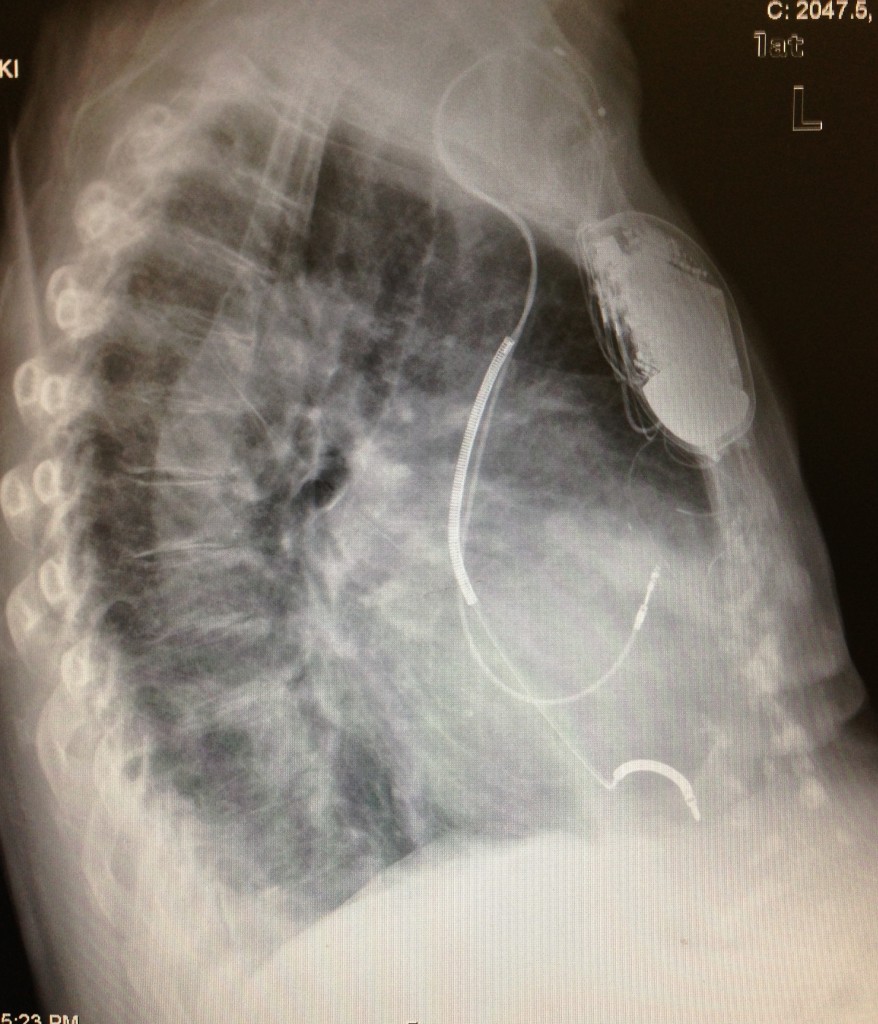
Please interpret the EKG and CXR and post your interpretations as well as your top diagnosis. Bonus points for including the correct next step in management. Feel free to discuss your DDx but credit will only be given for your top diagnosis.
nchristopher
Latest posts by nchristopher (see all)
- What’s wrong with this picture? – Answer - September 11, 2013
- What’s wrong with this picture? - August 21, 2013
- EKG Case 8 – Answer - July 16, 2013
- EKG Case 8 – All that wheezes - June 19, 2013
- EKG Case 7 Answer - June 19, 2013
9 comments for “What’s wrong with this picture?”