
Thanks for all the responses! Here is short version of the answer for those of you with ADD. Keep on reading for the details!
Our patient had sick sinus syndrome with a sinus bradycardia on top of her malfunctioning pacemaker. She was admitted to medicine for CHF exacerbation. The inpatient team obtained records from her cardiologist showing a paced rhythm on her last EKG within the month. EP was consulted to interrogate the pacer. When they came to evaluate the patient, she was found to be bradycardic to the 40s with a systolic BP in the 80s. A transvenous pacer was emergently placed and the patient was admitted to the CCU. Her pacemaker settings were adjusted and the following EKG was obtained showing atrial pacing prior to discharge.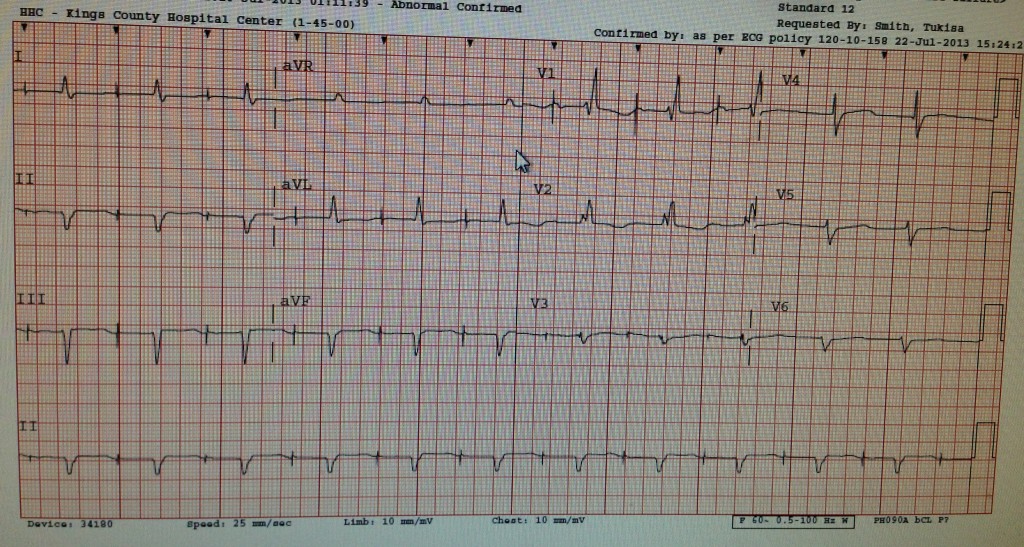
EKG
Rate = counting out the rhythm strip you see 10 ventricular beats, which corresponds to a rate of 60. If you look at the beat to beat variability, there are some gaps that would give you a rate just below 50.
Rhythm = The beats seem to come in couplets, however, the timing between each ventricular beat is not consistent. The key to this EKG is to look for P waves, which are very difficult to find but they are there. Specifically if you look in the rhythm strip the 2nd, 5th, 6th and 8th beats have visible P waves. You can also see a P wave before the first ventricular complex in V1 and V2 as Joey pointed out. The fact that there are some P waves present in the setting of an a wide complex rhythm brings up the potential of a 3rd degree heart block, but you don’t really see the classic P waves marching through the QRS complexes. Furthermore, the PR interval for those P waves that are visible is not significantly changing. Thus the rhythm is a sinus bradycardia with a possible underlying diagnosis of sick sinus syndrome.
If you didn’t notice those P waves, you could easily call this afib with a slow ventricular rate. The fact that its irregular makes it less likely to be a junctional escape or ventricular escape rhythm.
One thing many people noted in their interpretation was Ventricular Bigeminy. However, bigeminy should look like this:

With every other beat being a PVC that has a significantly different conduction pathway than the prior beat.
Axis = LAD with LAFB
Intervals = wide QRS complexes with RBBB and when the P waves are present the PR interval is just at the borderline of normal (200ms). The QTc is about 460ms which is slightly long
ST segments and T waves = Typical pattern of T wave discordance seen in RBBB (T waves take the opposite deflection when compared to the QRS), but no ST segment depression or elevation. Single flat T wave in lead I.
Chambers = no signs of LVH or atrial enlargement.
CXR
In order to really understand this case, we need to know about pacemakers and what they look like on imaging. Based on the type and number of leads as well as their location we can figure out what type of pacemaker it is and what it should be doing.
Dan referenced a great review. Breifly, here’s what you should look for when evaluating a pacer/ICD
AICD/Pacer
 Most commonly our CHF patients with low EF (<35%) will have an AICD. Modern AICDs have a backup pacing mode as well. You can identify an AICD by the fact that its lead will have two areas of the wire which look thicker. These areas are the shock coils. If there are no changes in the thickness of the wire, then the device is a single chamber pacer.
Most commonly our CHF patients with low EF (<35%) will have an AICD. Modern AICDs have a backup pacing mode as well. You can identify an AICD by the fact that its lead will have two areas of the wire which look thicker. These areas are the shock coils. If there are no changes in the thickness of the wire, then the device is a single chamber pacer.
Dual Chamber Pacer
 A second type of pacer is a dual chamber. This pacer has one lead in the right atrium and a second in the right ventricle. It has the ability to sense and pace both chambers. It may also include and ICD function.
A second type of pacer is a dual chamber. This pacer has one lead in the right atrium and a second in the right ventricle. It has the ability to sense and pace both chambers. It may also include and ICD function.
Biventricular Pacer
 A biventricular pacer will have one lead in the right ventricle and a second lead that courses through the coronary sinus and into a vein on the wall of the left ventricle. Biventricular pacing is used for Cardiac Resynchronization Therapy in heart failure patients with a LBBB.
A biventricular pacer will have one lead in the right ventricle and a second lead that courses through the coronary sinus and into a vein on the wall of the left ventricle. Biventricular pacing is used for Cardiac Resynchronization Therapy in heart failure patients with a LBBB.
Biventricular Dual Chamber ICD/pacer
 Lastly a dual chamber biventricular pacer has a right atrial lead, right ventricular lead and left ventricular lead that courses through the coronary sinus. Shock coils are again seen. The course of the left ventricular lead is more clearly seen on the lateral film.
Lastly a dual chamber biventricular pacer has a right atrial lead, right ventricular lead and left ventricular lead that courses through the coronary sinus. Shock coils are again seen. The course of the left ventricular lead is more clearly seen on the lateral film.
Looking at our patients CXR, she seems to have a dual chamber ICD with one lead in the right atrium and another in the right ventricle. There is a third lead that is coming off the pacer and ends in the left chest wall. This is likely the left ventricular lead that was either never implanted correctly or was displaced after implantation. Patients with Twiddler’s syndrome can actually pull back the pacemaker lead by spinning the generator under the skin.
Knowing the type of pacer helps, but now we need to figure out if it should be firing. This depends on the MODE of the pacer. This is represented by 3 letters defined by I-III in the table below:
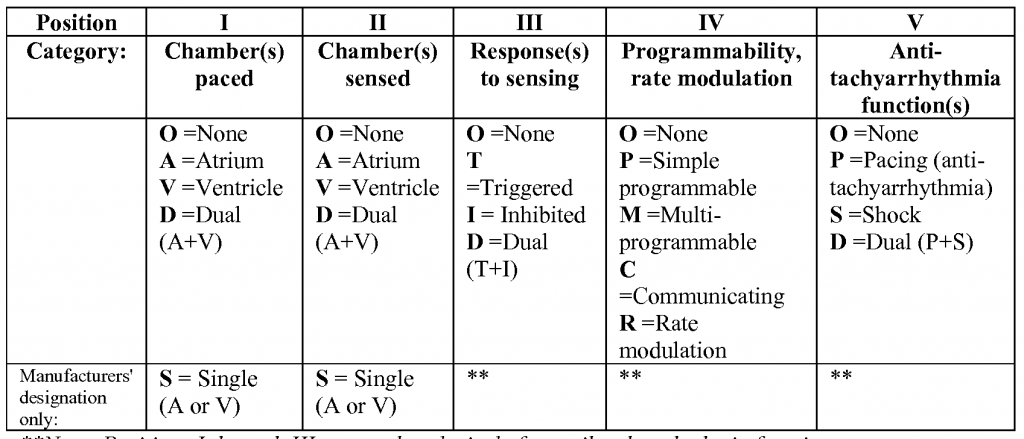
The most common mode for single chamber pacers is VVI or AAI.
- VVI = ventricular sense, ventricular pace, inhibit pacing if an intrinsic ventricular beat is sensed
- AAI = atrial sense, atrial pace, inhibit pacing if an intrinsic atrial beat is sensed
For dual chamber pacers, the most common mode is DDD which means both atria and ventricle are sensed. This can result in 4 possible patterns:
- If there is a sinus beat with normal AV conduction at a rate faster than the minimum set rate of the pacer, the pacer is inhibited
- If there is sinus bradycardia with normal AV conduction the atria will be paced and conduction will follow the normal pathway and generate a ventricular beat
- If there is slow or absent conduction through the AV node the pacer will sense each atrial beat and provide ventricular pacing
- If there is sinus bradycardia with absent AV conduction both the atria and ventricles will be paced
With the above in mind, looking at the EKG and CXR together, our patient has sinus bradycardia which means that the pacer should be either pacing the atria or ventricles or both. (Assuming the minimum set rate is above 60 BPM). Given the presence of P waves with an irregular bradycardia the patient likely has sick sinus syndrome.
nchristopher
Latest posts by nchristopher (see all)
- What’s wrong with this picture? – Answer - September 11, 2013
- What’s wrong with this picture? - August 21, 2013
- EKG Case 8 – Answer - July 16, 2013
- EKG Case 8 – All that wheezes - June 19, 2013
- EKG Case 7 Answer - June 19, 2013