
Today’s Morning Report is presented by Dr. Brown!
Recommendations for Management of First-time Seizure and Status Epilepticus
1. Are we mandated to report to DMV?
– no, but other states (CA, DE, NV, NJ, PA) have mandatory reporting laws.
2. Which AED’s can you measure blood levels?
– phenytoin, carbamazepine, phenobarbital, and valproic acid
– levetiracetam levels cannot be checked in the ED
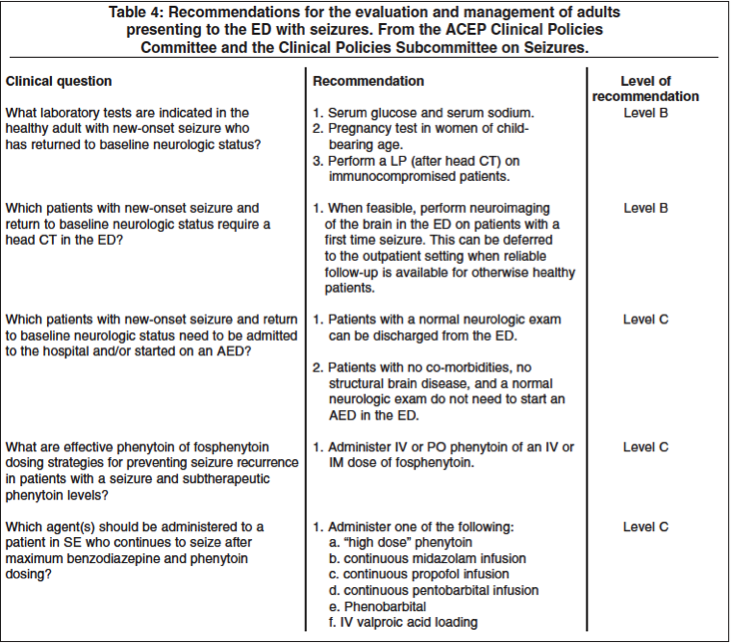
3. What are effective dosing strategies for preventing seizure recurrence in a patient found to have subtherapeutic serum phenytoin level?
– Level C recommendations:
- Give IV or oral loading dose of phenytoin
- Give IV or IM fosphenytoin
– There are no RCT comparing IV vs. PO loading doses
4. How should AED’s be loaded?
– Phenytoin can be loaded orally if given in appropriate doses (19mg/kg in men and 23mg/kg in women)
– Fosphenytoin 15-20 PE/KG IV or IM
– Valproic acid 20mg/kg
– Levetiracetam, cannot be readily checked, but because of wide therapeutic index, considered safe to give w/o knowing compliance
5. Ecclampsia: new onset GCT seizure during pregnancy or up to 4 weeks post partum
– Mg loading dose of 4-6g over 20 minutes with maintenance infusion of 1-2g/hour
- If continue to have seizure activity, give benzos
6. Trauma: 4% of epilepsy is caused by trauma. The risk of post-traumatic seizures is directly related to the severity of injury, but is not affected by early use of AED.
Status epilepticus: continuous or intermittent seizures for more than 5 minutes without recovery of consciousness
– after 5 minutes, seizures become:
- less likely to spontaneously terminate
- less likely to be controlled by an AED
- more likely to cause neuronal damage.
– RSI: give short-acting paralytic to prevent masking ongoing seizure activity
– Benzodiazepines are first line treatment
- 2mg IV every 2 minutes x 5 doses (10mg total)
Fosphenytoin is second-line treatment (lacks propylene glycol diluent)
– 20mg/kg, another 10mg/kg bolus can be considered
*** failure to respond to benzodiazepine and phenytoin defines refractory status epilepticus. 9-30% of status becomes refractory, and mortality jumps to 50%.
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015