
Here’s Dr. DiMare with another Morning Report!
Fibrinolytics for Suspected PE in Cardiac Arrest
tPA in cardiac arrest seems like a great idea
– 81% are from MI and PE
– only 2-10% survival in out of hospital arrest
When should you give it?
– Current literature is favorable only in patients with known PE
– BUT. . . ACLS guidelines say its ok in presumed PE…
– What should make us think PE above other causes such as MI?
- Bedside echo? If you have ROSC long enough to take a look
- Based on rhythm? More likely PEA and asystole
- Labs? Profound lactic acidosis
- EKG? R heart strain
– “Not enough evidence to support routine use in undifferentiated cardiac arrest…”
Whats the dose? How should you give it?
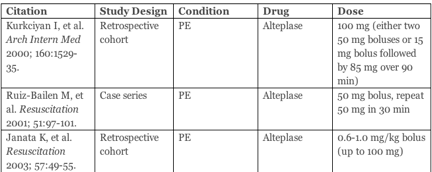
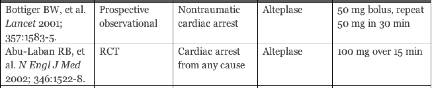
What happens next?
– continue CPR for 15-30 minutes
– consider a 2nd bolus dose of 50mg
– heparin should be started
- LMW vs UF?
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.




Jay Khadpe MD
Editor in Chief of "The Original Kings of County"
Assistant Professor of Emergency Medicine
Assistant Residency Director
SUNY Downstate / Kings County Hospital
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015