
Hope everyone had a happy Thanksgiving holiday weekend! Dr. Adal is back today with Morning Report!
Priapism
Definition
A persistent erection of the penis or clitoris that is not associated with sexual stimulation or desire.
Epidemiology
Incidence of 0.73 per 100,000 men each yr. Has a bimodal distribution of incidence, between 5-10 in children, and 20-50 in adults. More common in Sickle Cell population, with up to 45% of patients experiencing priapism at some point throughout their life.
Anatomy
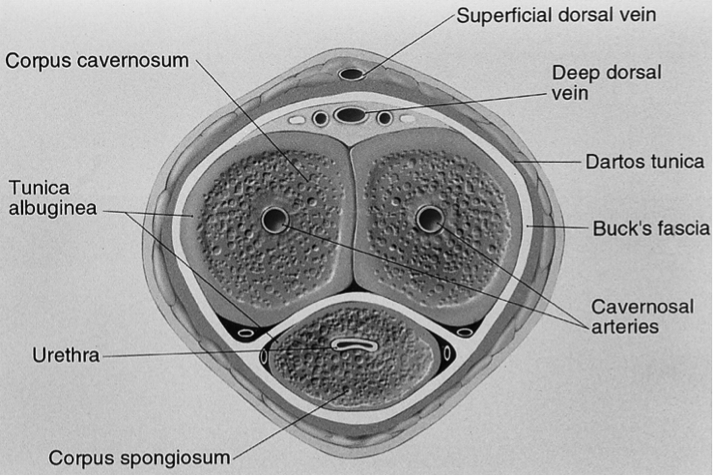
Pathophysiology
The precise mechanism of priapism is unknown. Persistent obstruction of venous outflow vs excess arterial inflow
Ishemic/Low flow priapism:
Characterized by little or no cavernous blood flow and abnormal cavernous blood gases (hypoxic, hypercarbic, and acidotic).
The corpora cavernosa are rigid and tender to palpation.
Patients typically report pain.
Non-ischemic/High flow priapism:
Caused by unregulated cavernous arterial inflow.
Cavernous blood gases are not hypoxic or acidotic.
Typically the penis is neither fully rigid nor painful.
Antecedent trauma is the most commonly described etiology.
Nonischemic priapism does not require emergent treatment.
Stuttering/Intermittent:
Recurrent form of ischemic priapism
Repeated episodes of painful erections with intervening periods of detumescence.
Common in sickle cell patients and can lead to true ischemic priapism
Eitiology
| Hematologic (sickle cell anemia, leukemia, thalassemia, multiple myeloma, thrombotic thrombocytopenic purpura) |
| Neurologic (spinal shock) |
| Tumors (metastatic cancers) |
| Perineal, pelvic or penile trauma |
| Iatrogenic (intracavernous injections) |
| Drugs (anticoagulants, anti-hypertensives, anti-depressants, PDE5 inhibitors, intracavernous injections, alpha-blockers, cocaine) |
| Infection (malaria, spider toxins) |
| Metabolic disorders (gout, hemodialysis, high lipid content, total parenteral nutrition, diabetes, amyloidosis) |
Diagnosis
H&P, Blood Gas, Duplex ultrasound
Ischemic:
Corpora fully rigid, pain, no evidence of trauma
Blood gas will have dark color. Ph < 7.25, pO2 <or= 40, pCO2 >or=60
Doppler ultrasound will reveal little or no flow
Non-ischemic:
Corpora aren’t fully rigid, absence of pain, might have evidence of pelvic trauma
Blood gas not as dark. Ph >7.25, pO2 <or= 60, pCO2 >or=40
Doppler ultrasound will reveal normal or high flow, might reveal vascular abnormalities
Consider other lab tests: CBC, retic, tox screen, Hgb electrophoresis
Management Algorithm
Ischemic
1. Aspiration with or without irrigation (normal saline). Success rate about 30%. Enter corpora at 10 or 2 pm, to avoid the dorsal nerve arteries, vein and urethra
2. Phenylephrine injection [100 -500mcg/ml] 58% successful if done alone, 77% if followed by step 1. Patients should be on a cardiac monitor
3. Surgical shunting
Non-ischemic
1. Observation vs close follow up with Urology
2. Arteriography or embolization
3. Surgical ligation
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015