
Brought to you by Dr Andrew Grock and Dr. Elizabeth Abram. Supervised by Dr Martindale.
A nurse brings you the following EKG to sign.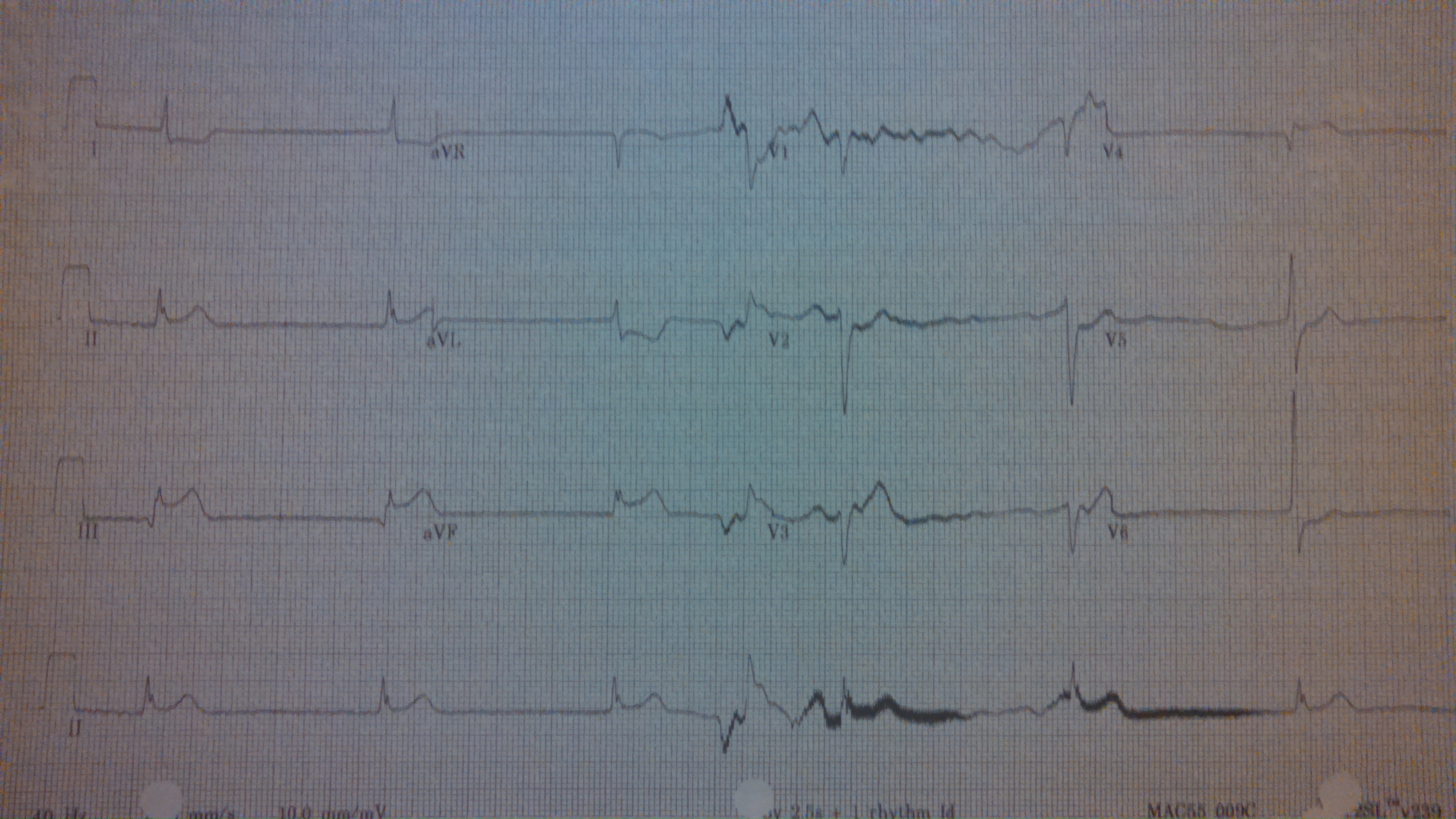 You go to the patient’s bedside:
You go to the patient’s bedside:
63 yo F, pmhx dm/htn, here for epigastric pain, vomiting, dizziness x 4 hours. She is diaphoretic and reporting active pain and nausea at this time.
To win the week’s prize please provide the following:
1. Full interpretation of ekg including rate, rhythm, axis, intervals, st-t segments, t- wave interpretation, other
2. Please explain pathophysiology of the ekg abnormality or abnormalities featured above
3. Please provide the appropriate sequence of treatment actions in caring for this patient.
4. Which common treatment for this problem is contra-indicated?
The answer will be posted next Friday!
andygrock
- Resident Editor In Chief of blog.clinicalmonster.com.
- Co-Founder and Co-Director of the ALiEM AIR Executive Board - Check it out here: http://www.aliem.com/aliem-approved-instructional-resources-air-series/
- Resident at Kings County Hospital
Latest posts by andygrock (see all)
- A Tox Mystery…. - May 26, 2015
- Of Course, US Only for Kidney Stones… - May 18, 2015
- Case of the Month 11: Answer - May 12, 2015
- Too Classic a Question to Be Bored Review - May 5, 2015
- Case of the Month 11: Presentation - May 1, 2015
5 comments for “6/13/14 EKG #10…this one is scary”