
By Dr. Kelly Maurelus.
Hey Folks, I am bringing you the Ultrasound image of the month or in this case video of the month…take a moment and review the media (click play as many times as you want) to come up with the diagnosis.
What is your diagnosis?
If you look closely some physicians may note initially a gestational sac with fetal pole at the beginning of the clip, which can also be seen in IMAGE 1. Usually you remove the probe and call it a day; however, if you continue to fan through the entire structure you will notice that this so called IUP is not in the uterus but the adnexa and there is a normal IUP within the uterus, IMAGE 2 – this is known as a heterotopic pregnancy!

Image 1 showing adnexa with extrauterine pregnancy
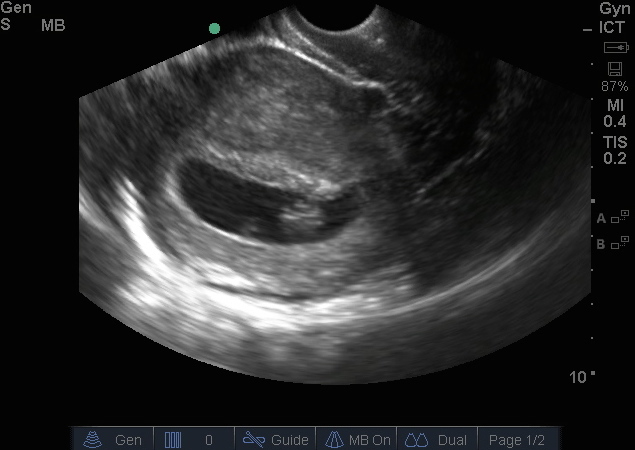
Image 2 showing normal intrauterine pregnancy
Heterotopic pregnancies are very rare indeed, occurring in approximately 1:30,000 pregnancies; the incidence is much higher due to assisted reproduction as it rises to 1:7,000 overall and can be as high as 1:900 with ovulation induction. They are defined as the co-existence of intrauterine and extrauterine gestation. Given its rarity a heterotopicc gestation is difficult to diagnose clinically. It should definitely be considered more likely in the following circumstances:
-Assisted reproduction techniques
-Persistent or rising beta-hCG levels after D+C
-Uterine fundus larger than expected dates
-More than one corpus luteal cyst is present
Most common location of ectopic gestation in a heterotopic pregnancy is the fallopian tube albeit cervical and ovarian locations do occur but with much lower frequency. Majority of reported cases are of singleton intrauterine pregnancies. Both triplet and quadruplet heterotopics have been reported but are extremely rare but can be seen with assisted conceptions.
Mimics of heterotopic pregnancies include but are not limited to:
-Intrauterine gestation with hemorrhagic corpus luteum
-Bicornuate uterus with gestation in both cavities
-Acute abdomen during pregnancy such appendicitis and coincidental vaginal bleeding
Ultrasound is of course the modality of choice in diagnosing heterotopic pregnancies. In order to diagnose it one must look at the adnexa since most will be in the area of the fallopian tubes; the tubes themselves are hard to visualize on ultrasound unless the patient has hydrosalpinx.
The high-resolution endocavitary probe is most useful to diagnose heterotopic pregnancies; as always try to first visualize the pelvis with the phased array cardiac probe or curvilinear abdominal probe. Make sure to obtain a global image first of the uterus and then scan through the entire structure. You will see an intrauterine pregnancy defined as a gestational sac with either a yolk sac or fetal pole with heart beat BUT DO NOT STOP THERE!
Always try to visualize the adnexa for ovaries looking for a complex cystic structure or you may just find another gestational sac with a yolk sac or fetal pole. Ovaries may be difficult to visualize especially in our patient population but just remember to LOOK FOR THE CHOCOLATE CHIP COOKIE! The ovaries are medial and anterior to your iliac vessels, and will have a hyperechoic capsule with anechoic or black round follicles in the middle. One of those follicles may be larger than the others and this is most likely the corpus luteal cyst. Try to view both ovaries in two planes both sagittal and coronal and look for any associated free fluid as this may represent a ruptured ectopic.
Treatment of heterotopic pregnancies remains a challenge as serial beta-hCG levels are not useful in the diagnosis and medical management with methotrexate is contraindicated with an intra-uterine pregnancy. Standard care remains laparoscopy/laparotomy to remove the tubal pregnancy while minimally manipulating the uterus to preserve the intrauterine pregnancy.
Key Points to Remember
–If you don’t think about heterotopic you will not diagnose it
-Always look at the adnexa even if you find an IUP
-Ovaries look like chocolate chip cookies, medial and anterior to iliac vessels
-Higher incidence of heterotopic in assisted reproduction patients
References:
Michał M, Marian M, Marek M, Ewa WO. Heterotopic pregnancy in the absence of risk factors-diagnostics difficulties. Ginekol Pol. 2011 Nov;82(11):866–68.
Simsek T, Dogan A, Simsek M, Pestereli E. Heterotopic triplet pregnancy (twin tubal) in a natural cycle with tubal rupture: case report and review of the literature. J Obstet Gynaecol Res. 2008 Aug;34(4 Pt 2):759–62.
Gruber I, Lahodny J, Illmensee K, Losch A. Heterotopic pregnancy: Report of three cases. Wien KlinWochenschr. 2002;114:229–32.
Sohail S. Hemorrhagic corpus luteum mimicking heterotopic pregnancy. J Coll Physicians Surg Pak. 2005;15:180–81.
Kriplani A, Lunkad AS, Sharma M, Ammini AC. Recurrent ectopic pregnancy with heterotopic pregnancy in a patient of hypo gonadotropic hypogonadism: a case report. J Reprod Med. 2011 May-Jun;56(5-6):274–76.
Varras M, Akrivis C, Hadjopoulos G, Antonion N. Heterotopic pregnancy in natural conception cycle presenting with tubal rupture: a case report and review of literature. Eur J Obstet Gynecol Reprod Biol. 2003;(106):79–82.
andygrock
- Resident Editor In Chief of blog.clinicalmonster.com.
- Co-Founder and Co-Director of the ALiEM AIR Executive Board - Check it out here: http://www.aliem.com/aliem-approved-instructional-resources-air-series/
- Resident at Kings County Hospital
Latest posts by andygrock (see all)
- A Tox Mystery…. - May 26, 2015
- Of Course, US Only for Kidney Stones… - May 18, 2015
- Case of the Month 11: Answer - May 12, 2015
- Too Classic a Question to Be Bored Review - May 5, 2015
- Case of the Month 11: Presentation - May 1, 2015