
EKG July 2014
45 yo nulliparous F of Hispanic and Caucasian descent pmhx HTN on longstanding ARB p/w left intermittent arm pain x 1 year and 2 days of worsening mid back discomfort and SOB. Pt regularly walks 5 miles a day and has a BMI of 22. Had a benign bladder polyp resected 3 months prior and since then has entered perimenopause with irregular menses. Denies nausea/vomiting/diaphoresis. No other medical problems or environmental exposures.
SH: occasional ETOH (1-2 glasses of wine/wk), no smoking or illicits
FH: one aunt deceased prior to age 50, no known CAD
VS: 152/98, HR 72, RR 16, SaO2 100%, afebrile
PE otherwise unremarkable… except you note the patient seems rather flexible for her age.
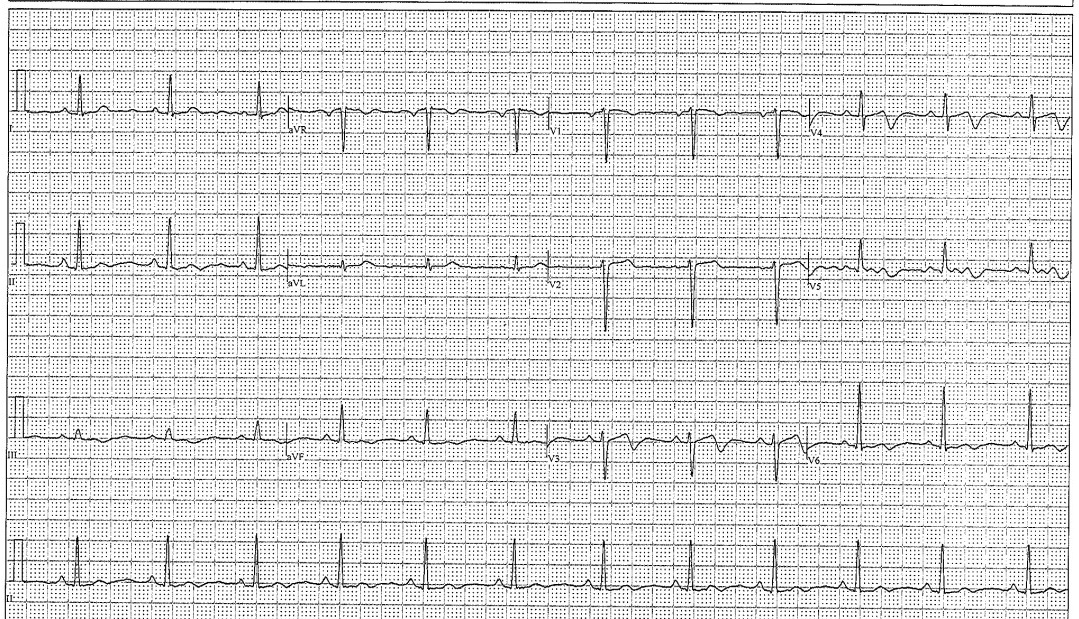
EKG as above.
CXR unremarkable.
This patient was sent from her PMD via ambulance for the above abnormal EKG.
- What about this EKG is concerning?
- After a troponin of 1, Cardiology does a bedside echo and discovers wall-motion abnormalities. The patient is taken to cardiac cath. No plaques are seen, yet stents are placed. What is the location(s) of the stents?
- What is this condition called?
- What are some of the underlying conditions that may have pre-disposed this patient to her diagnosis?
Now is your chance to figure out what was going on! Best answer to the above 4 questions by noon Friday 7/18/14 wins.
By Dr. Elizabeth Abram
Supervised by Dr. Jennifer Martindale.
eabram
Latest posts by eabram (see all)
- Rhythm Nation May 2015 Answer! - June 1, 2015
- Rhythm Nation May 2015 - May 10, 2015
- Rhythm Nation April 2015 – Answer! - April 20, 2015
- Rhythm Nation April 2015 - April 13, 2015
- Rhythm Nation March 2015 – Answer! - March 31, 2015
4 comments for “Rhythm Nation July 2014”