
Hey everyone! Hope you enjoy this month’s Ultrasound of the Month and my first official blog post!
Here’s the clip:
A 45 year old man presented to UHB fast track with a chief complaint of right knee pain. His pain began 4 days ago after a hyperflexion injury. He had immediate pain and swelling and has had difficulty walking since.
On exam you found the patient to have a large suprapatellar effusion. He was unable to extend his knee against gravity or to control flexion of his knee against gravity when it was passively extended for him. While the entire knee was mildly tender, he had no discrete bony tenderness.
You get an x-ray…
…it confirms your physical exam finding of a large suprapatellar effusion.
Now what?(HINT: this is an ultrasound blog post)
A.Call ortho
B. Put the patient in an immobilizer, give him some crutches and send him to ortho clinic
C. Get a CT scan
D. Do an ultrasound
You are an awesome Clinical Monster and decided to do an ultrasound which confirmed your suspected diagnosis of ….. (partial) QUAD TENDON RUPTURE!
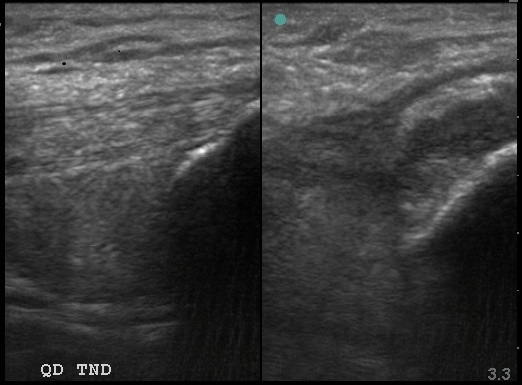
Left: normal Right: abnormal
According to the American Academy of Orthopedic Surgeons, quadriceps tendon ruptures (QTR) tends to occur in two, predominantly male groups. The first – isolated traumatic rupture – occur infrequently and in a middle aged population. These injuries are usually associated with playing a running or jumping sport. The second, and much larger group, occur either in the setting of minor trauma or are idiopathic and happen most frequently to patients in the 6th or 7th decade of life. These patients often have some underlying decrease in vascular flow to the region and/or additional comorbid conditions such as diabetes, gout, hypothyroidism or chronic steroid injections.
Because of the large amount of swelling associated with QTR, diagnosis solely based on physical exam is limited and is largely dependent on imaging. Previously, in the ED, XR was the only imaging modality offered. Occasionally XR would show the affected patella in a low lying position when compared to the contralateral patella. However, this finding was not sensitive or specific for QTR. The gold standard of imaging for QTR remains MRI. However, this is clearly difficult to obtain in the ED. If only we had another option… like US!
The quadriceps tendon is formed by the convergence of four muscle tendons:the rectus femoris, vastus medialis, vastus intermedius and vastus lateralis. On ultrasound, these tendons appear as a 6 to 11 mm3 thick band with parallel echoes forming three distinct layers. Partial QTR can involve a single or multiple layers while a complete QTR involves all three.
Ultrasound can not only identify the presence or absence of a rupture but also identify whether one is complete are partial. In complete tears, a hypoechoic or anechoic area between the tendon fibers is usually seen, and is usually representative of a hematoma. Partial tears may display a focal hypoechoic defect in the tendon.
Making a diagnosis at the bedside during a patient’s ED visit is not only gratifying, but it can have a direct positive effect on the patient’s treatment and overall outcome. Full QTR requires surgery, often in an urgent manner. Early repair allows end to end repair of tendons as well as tendon to bone anchorage. In some cases, partial QTR can be managed conservatively but full range of motion can most often be achieved with prompt immobilization and initiation of treatment. Given the difficulty of making the diagnosis of a partial QTR, bedside sono can be used to ensure proper initiation of treatment on initial presentation.
By Dr. Michelle DiMare
Thanks for reading!
- Secko M, Diaz M, Paladino L Ultrasound diagnosis of quadriceps tendon tear in an uncooperative patientJ Emerg Trauma Shock. 2011 Oct-Dec; 4(4): 521–522.
- La S, Fessell DP, Femino JE, Jacobson JA, Jamadar D, Hayes C. Sonography of partial-thickness quadriceps tendon tears with surgical correlation. J Ultrasound Med. 2003;22:1323–9.
- Zeiss J, Saddemi SR, Ebraheim NA. MR imaging of the quadriceps tendon: Normal layered configuration and its importance in cases of tendon rupture. AJR Am J Roentgenol. 1992;159:1031–4.
andygrock
- Resident Editor In Chief of blog.clinicalmonster.com.
- Co-Founder and Co-Director of the ALiEM AIR Executive Board - Check it out here: http://www.aliem.com/aliem-approved-instructional-resources-air-series/
- Resident at Kings County Hospital
Latest posts by andygrock (see all)
- A Tox Mystery…. - May 26, 2015
- Of Course, US Only for Kidney Stones… - May 18, 2015
- Case of the Month 11: Answer - May 12, 2015
- Too Classic a Question to Be Bored Review - May 5, 2015
- Case of the Month 11: Presentation - May 1, 2015