
47 years old male with no PMH presents with one day of severe epigastric pain. States that he had this type of pain before, and his PMD prescribed him “some pills” that helped with the pain. But he no longer takes the medication. You get a CXR and you see…
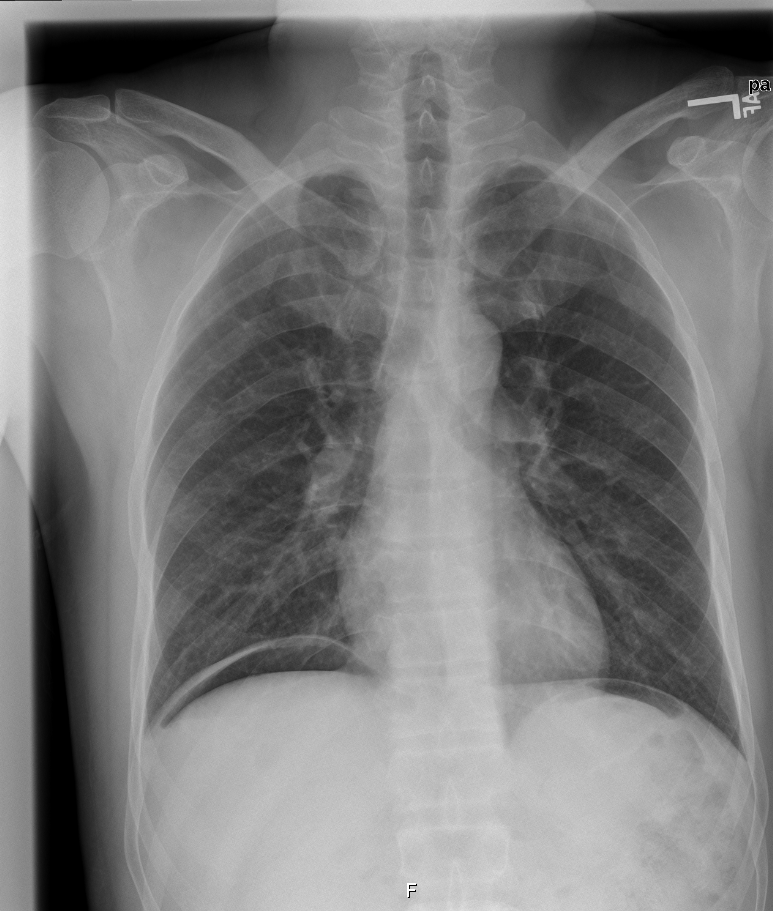
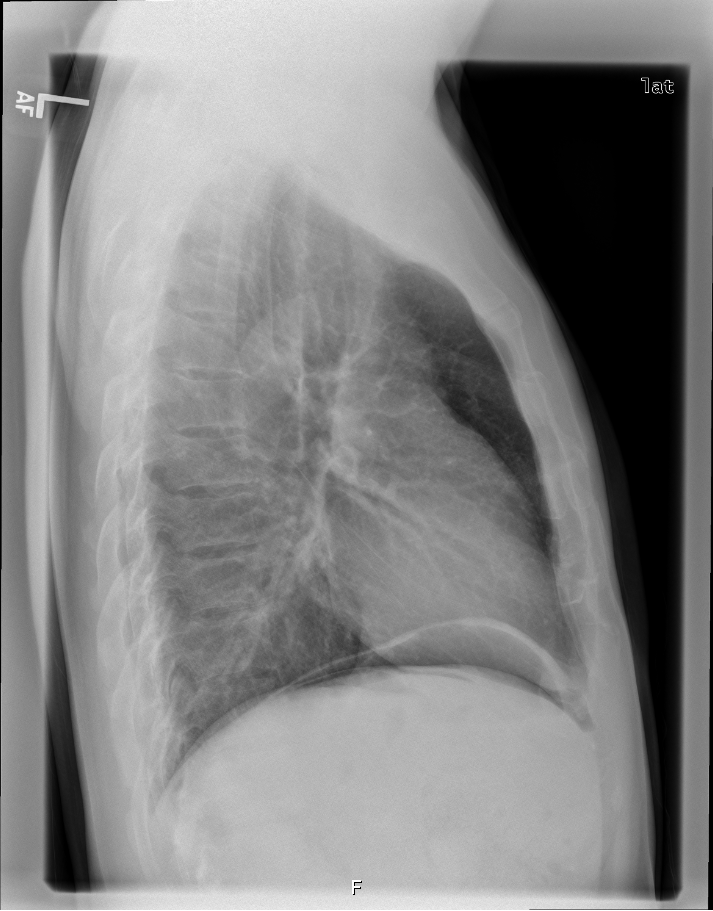
please interpret the CXR. what’s on your differential diagnosis? what the most likely diagnosis? how are you going to manage this patient?
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

jwang
Latest posts by jwang (see all)
- Xray Vision Answer - May 24, 2015
- Xray Vision: My Arm Looks Funny…. - May 16, 2015
- Xray Vision: Limping Answer - April 27, 2015
- Xray Vision: Limping - April 17, 2015
- Xray Vision: Answer - March 27, 2015
2 comments for “XRay Vision: So Much Abdominal Pain”