
Here are the images again

Both Drs. Greenstein and Chan got the answer right. Dr. Greenstein is the winner for putting in the read first. Please note that there is a fracture noted on the post reduction film.
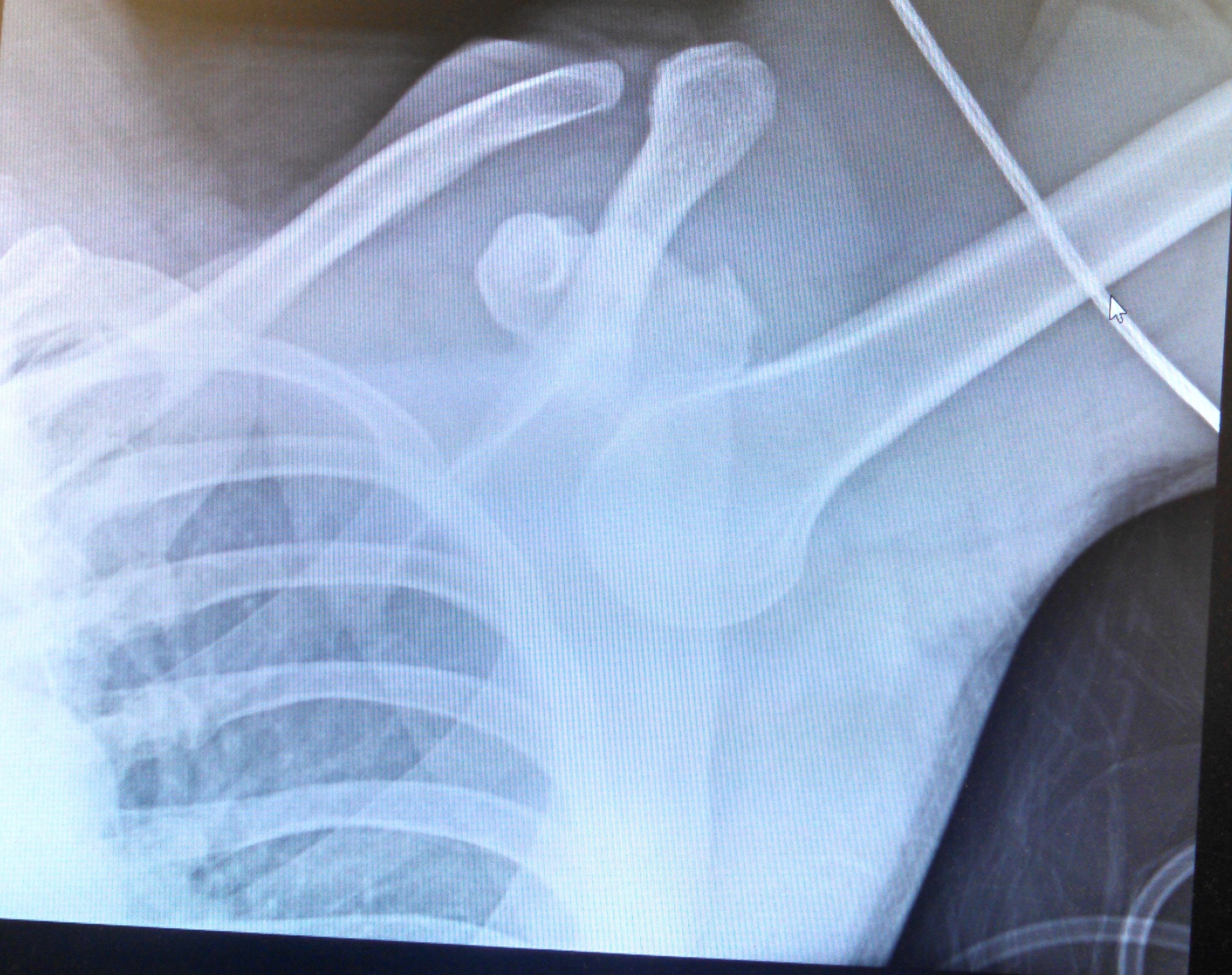
Answer:
1st Xray: read as inferior shoulder dislocation.
2nd Xray: Post reduction of the dislocation. However, there is a fracture at the superolateral humeral head (compatible with Hill-Sachs fracture).
Inferior Shoulder Dislocations (Luxatio Erecta)
Uncommon. Counts of less than 1% of shoulder dislocations. Results from forceful hyperabduction of the shoulder. The hyperabduction causes the impingement of the humeral head again the acromion. The inferior capsule tear and the humeral head is displaced inferiorly. Often associated with significant soft tissue trauma or fracture.
Clinical features:
Patient typically presents with affect shoulder in a “locked” position (hyperabducted). Usually, humerus fully abducted, elbow flexed, and hand behind the head.
Exam:
Perform a neurovascular exam prior to and post reduction to assess nerve or vascular injuries.
Test the axillary nerve by assessing sensory over the deltoid
Radial nerve can be test by examining the strength of wrist extension.
Assess distal pulses and cap refill before and after reduction.
Reduction Methods:
Axial (in line) traction method:
Place patient in supine position.
One operator stands by the patient’s head and apply axial traction inline with the abducted arm. Second operator can assist by providing countertraction using a sheet wrapped diagonally over affected shoulder. After reduction, patient should be able to fully adduct against chest wall. Then, place patient in sling for post reduction films.
Two-step reduction method:
Step One: convert to anterior dislocation – the operator stands on affected side by the patient’s head. One hand on the lateral aspect of mid-humerus, the other on medial condyle. Push anteriorly with the hand on mid-humerus at the same time pull posteriorly with hand on medial condyle. This will convert inferior dislocation to anterior.
Step Two: Reduction of anterior dislocation – adduction and external rotation.
Place in sling. Post reduction film.
Complications:
Brachial Plexus Injury: 50-60% of patient with inferior shoulder dislocation have associated brachial plexus injury. Examine and document neurovascular exam pre/post reduction.
Rotator cuff tears.
Associated fractures of glenoid rim, greater tuberosity, acromion, clavicle and coracoid process. These fracture can occur from the dislocation or with repeat reductions.
By Dr. Joyce Wang
References:
Anantha, Malia, and Erik Schraga. “Joint Reduction, Inferior Shoulder Dislocation.” Inferior Shoulder Dislocation. EMedicine, 3 Jan. 2012. Web. 25 Sept. 2014. <http://emedicine.medscape.com/article/110422-overview#a17>.
Rudzinski J.P., Pittman L.M., Uehara D.T. (2011). Chapter 268. Shoulder and Humerus Injuries. In Tintinalli J.E., Stapczynski J, Ma O, Cline D.M., Cydulka R.K., Meckler G.D., T (Eds), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e.
jwang
Latest posts by jwang (see all)
- Xray Vision Answer - May 24, 2015
- Xray Vision: My Arm Looks Funny…. - May 16, 2015
- Xray Vision: Limping Answer - April 27, 2015
- Xray Vision: Limping - April 17, 2015
- Xray Vision: Answer - March 27, 2015