
Well that was unexpected…
By Dr. Michelle DiMare
Welcome back! This month’s post explores a common diagnosis with an uncommon complication. Or is it more common than we think??
In a fictional hospital nearby, a healthy 20 something year old female is seen for chest pain x 5 days. As if reciting from a textbook, she tells you she recently had a cold. She reports gradually resolving cough and runny nose that were replaced by a centrally located chest pain that occasionally radiates to the back. The pain is worse when laying flat and improves when leaning forward.
Her VS are BP 117/67 HR 82 RR 20 (obviously) O2 100% and T 98.8
Her exam is basically unremarkable except for the fact that she prefers to sit with her body leaning forward. You think her heart sounds are normal but they’re tough to hear over the retching of the guy in the curtain next door.
Her EKG looks like this:
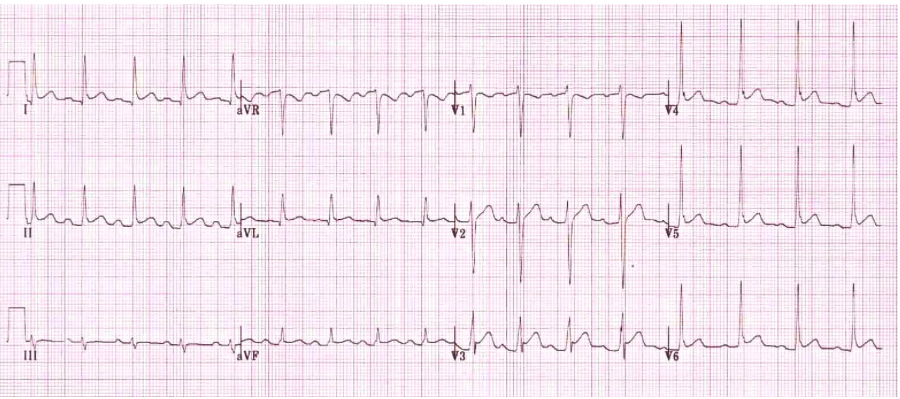
You see… widespread ST segment elevations with PR depressions and reciprocal ST depressions with PR elevation in aVR and V1
This further confirms this slam dunk diagnosis of… acute pericarditis.
Armed with a prescription for NSAIDs and a whole lot of reassurance, you’re about to discharge the patient when, out of the corner of your eye, you see the ultrasound. Clean, charged and begging to be used, you grab it and figure, “hey, I might as well teach the medical student something…”
Check out the clips below:
PSL
PSS
Apical 4
Subxyphoid
IVC
Well, that was unexpected…
Any bedside ultrasound should be done with the intention of answering specific questions. In the case of an echo on someone with pericarditis, the two questions we should always look to answer are:
- Is there a pericardial effusion?
- Are there signs of tamponade?
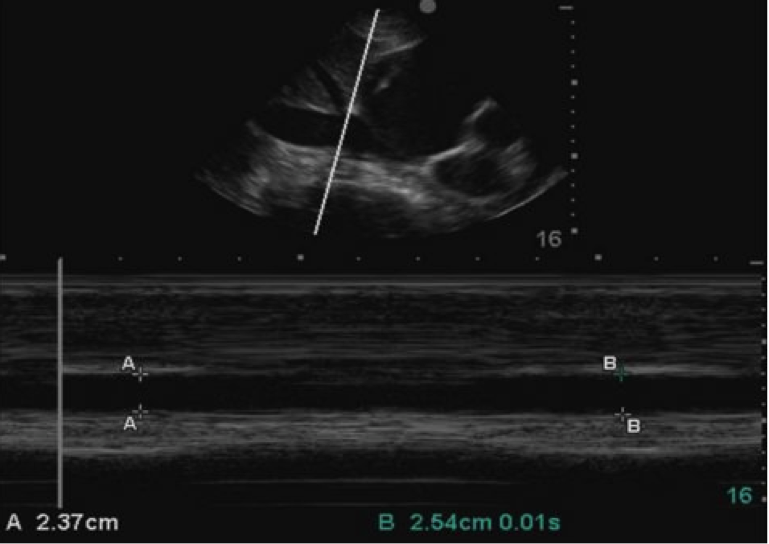
To answer question one. YES! There is a moderate pericardial effusion, seen in all 4 views. The effusion can be considered significant because it measures greater than 1 cm.
Question two is a little more difficult…
Clinically, the diagnosis of tamponade is indicated by Becks triad: muffled heart sounds, JVD and hypotension. Your mythical patient showed none of these signs but her ultrasound tells a different story.
2D Echocardiographic signs of tamponade:
- Presence of pericardial effusion
- Diastolic collapse of R ventricle
- IVC dilation and loss of respiratory variation
The apical four view only had a small amount of, if any, right ventricular collapse. However, the large effusion plus a dilated IVC with minimal respiratory variation is enough to prompt you to have a cardiologist see the patient and, at the first sign of instability, consider a pericardiocentesis.
Your patient was seen by cardiology and their “official” echo looked just like yours (hey, you’re pretty good at this ultrasound business) The patient was admitted to the CCU for “impending tamponade” and treatment of her acute pericarditis. On day 2 of her stay she was noted to have a steadily increasing heart rate and a steadily decreasing blood pressure, repeat echo showed further evidence of tamponade and CT surgery performed a pericardial window.
Take Home Points:
- If you don’t look for it, you’ll never find it
- ALWAYS add an IVC view
- A large IVC is the first, though non specific, finding in tamponade
- Don’t wait for clinical signs
- US can show early or “impending” tamponade
- This is a relatively new idea à formerly you either had tamponade or you didn’t
References:
http://lifeinthefastlane.com/ecg-library/basics/pericarditis/
https://web.stanford.edu/group/ccm_echocardio/cgi-bin/mediawiki/index.php/Tamponade
http://www.slredultrasound.com/Filesandpictures/Cardiac21.pdf
Jay Khadpe MD
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015