
Here are the images again:

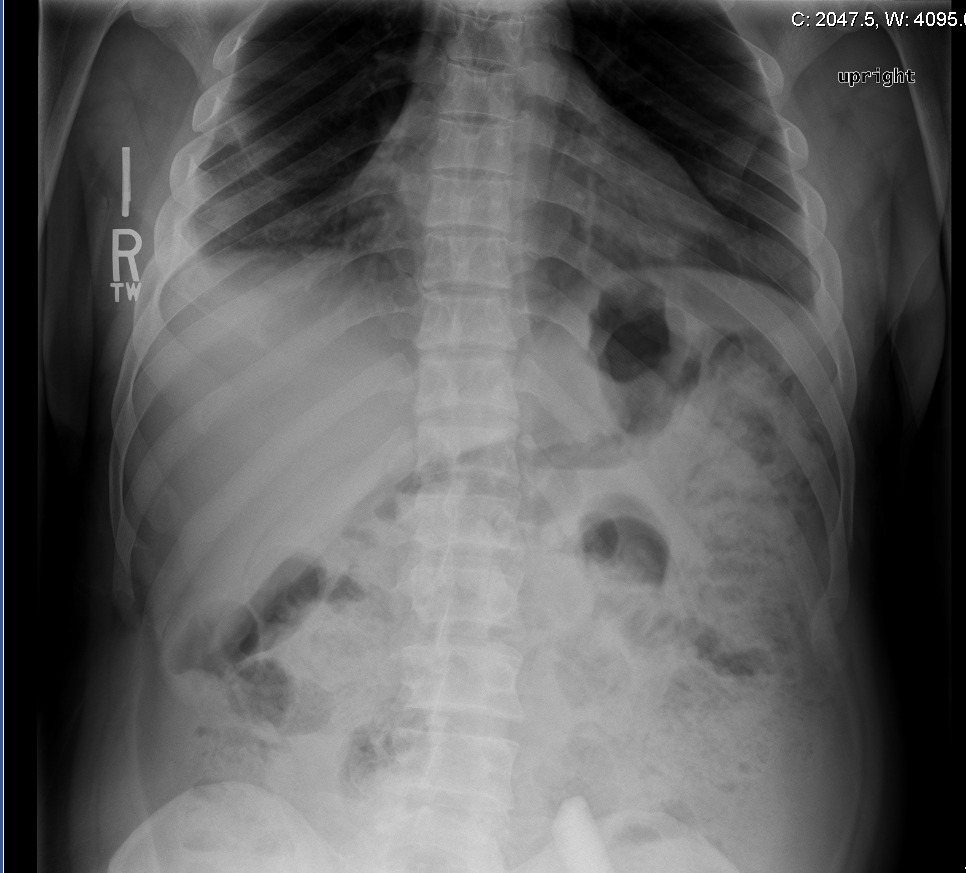
that’s correct Dr. Bogoch! it is indeed a domino! The patient was brought in by staff members of the facility after questionable ingestion during a game of dominos.
Ingested Foreign Body
Foreign bodies can be anywhere in the entire GI tract. The esophagus has three areas of narrowing where foreign bodies are most likely to become entrapped, at the upper esophageal sphincter (UES), the crossoer of the aorta, and the lower esophageal sphincter (LES). Certain structural abnormalities (strictures, webs, diverticula, or tumors) of the esophagus can increased the risk of foreign body entrapment.
If the foreign body reaches the stomach, it has > 90% of chance of passing. However, if the foreign body is > 2cm in diameter it is less likely to pass the pylorus. Objects >6cm can be entrapped at the pylorus or duodenal sweep. Once the foreign body gets into the small bowel it can be struck at the ileocecal valve.
Presentation:
Oropharyngeal foreign bodies: typically patients will endorse foreign body sensation due to the well innervation of the area. Rarely, patients have airway compromise, which is only seen with delay presentation with resulting infection or perforation. At times, foreign body can be visualized on physical exam.
Esophageal foreign bodies: Dysphagia and inability to tolerated secretion are typical complaints. In children, gagging, vomiting, and neck or throat pain are common presentations. In chronic esophageal foreign bodies in children, patients can presents with poor feeding, failure to thrive, stridor, or repetitive pneumonias from aspiration.
Stomahc/small intestine foreign bodies: typically presents with abdominal pain, vomiting or fever.
Imaging:
Plain radiographs are indicated for every patient with a known or suspected radiopaque foreign body in the GI tract. They can easily localize the object. Xray are typically done for patients who have swallowed bones even though the yield is low for patients who have swallowed bones.
CT is considered the imaging modality of choice to locate radiopaque foreign objects. CT with IV contrast is also indicated if a suspicious for perforation or abscess.
Endoscopy Indications:
Airway compromise
Patients who swallowed toothpicks or other sharp objects that are not visible on xrays but have high rates of complications (possible esophageal injuries).
If foreign body in the stomach o proximal duodenum is >2cm in diameter or longer than 5-7cm or oddly shaped foreign object.
Multiple magnets: as they can cause perforation, necrosis, fistula, volvulus, infection or obstruction.
Button battery in the esophagus.
Treatment
Monitor for airway compromise: drooling, inability to tolerate fluids, evidence of sepsis, perforation or active bleeding.
Button battery ingestion: if in the esophagus: URGENT endoscopy due to esophageal wall necrosis within 2 hours. Noted to be round radiopaque density with “double-contour” configuration. If in the stomach, endoscopy is typically not indicated. However, patients have to be monitor for disruption of the battery. Button batteries contain electrolyte solution and heavy metal, and if they break in the GI tract can cause heavy metal poisoning. Therefore, repeat xrays are indicated in 24-48 hours. If the battery is still in the stomach, endoscopy removal is necessary.
Objects localized on xray that are sharp, elongated (>5cm in esophagus, > 6cm in stomach/small intestine), multiple in number should be removed by endoscopy due to their high risk of perforation.
Disposition
Oropharngeal foreign bodies: if evaluation is negative in ED, discharge with follow up with ENT.
Esophageal foreign bodies: If foreign body noted in esophagus refer to GI for endoscopy. In stable children, if the coin is at the LES, return for repeat xray in 12-24 hours. If there is no advancement, refer for endoscopy.
Stomach/small intestine: if objects are <2cm in width or <6cm in length should be discharged home. Serial radiographs are generally not indicated. Discharge instructions should include return precautions for fever, vomiting or abdominal pain. Serial radiographs are indicated for sharp or large foreign bodies in the duodenum or small intestine. Follow up in 24 hours for repeat xray.
Case conclusion/management:
On plain xray noted to have the foreign body in the small intestine. Per radiology, the object is likely past the duodenal sweep. However, the foreign body measured to be 6.5cm. Therefore, patient was instructed to return to ED in 48 hours for repeat imaging. On repeat xray, the domino was noted to have passed into the large intestine.
References:
http://emedicine.medscape.com/article/776566-overview
http://www.uptodate.com/contents/ingested-foreign-bodies-and-food-impactions-inadultssource=search_result&search=ingested+foreign+body&selectedTitle=2~150
jwang
Latest posts by jwang (see all)
- Xray Vision Answer - May 24, 2015
- Xray Vision: My Arm Looks Funny…. - May 16, 2015
- Xray Vision: Limping Answer - April 27, 2015
- Xray Vision: Limping - April 17, 2015
- Xray Vision: Answer - March 27, 2015