
A 25 y/o smoker presents to the ED with SOB and tells you her asthma is acting up. You think to yourself, “I love the crashing asthma patient!” Within 5 minutes bipap is bedside, solumedrol is given and somehow she’s already on her 3rd round of combinebs. “Nailed it!”
She’s feeling pretty good now and breathing better. The room’s starting to get chaotic, but you’re a good doctor so you make sure to write her scripts for a course of oral corticosteroids and you even remember to say, “see your doctor in the next week” as she signs the discharge papers. Job well done!… right?
There are soooooooo many things missing here it hurts. Sure the course of steroids will cool everything off for a few more days, but what about a week from now when she’s back chain-smoking with her buds? Does she have albuterol at home? Is she going to see her PMD? Does she have a PMD??? Well you can ask her in 2 weeks when she comes back. (Catch my point?)
Controller versus Rescue medications
We know that asthma is a chronic inflammatory disease of the lungs. People with mild and occasional flares just use their albuterol and call it a day. However, for anyone using their albuterol more than 3 times/week. Their asthma is poorly controlled. It is time to start a controller medication to attack that ongoing inflammation. The first line and most effective controller medications are inhaled corticosteroids (1).
Yes! We can prescribe them and there is evidence that we should start prescribing these meds from the ED.
Rowe et al. published a placebo-controlled, double blind, RCT of 1,006 adult asthmatics being discharged from an ED in Canada and found that compared to placebo, patients who were started on an inhaled corticosteroid (Budenoside 400μg BID) had a 48% decrease in repeat hospital visits at 21 days, had better quality of life scores, had significantly less symptoms and used their albuterol inhalers almost 50% less than those in the placebo group. The placebo group had more adverse events (sorethroat and hoarsness) and an equal number of outcomes thought to be common with inhaled steroids (acne, fluid retention and insomnia).
NNT to prevent relapse was 9! (3)
Others who support starting inhaled steroids in the ED are:
- NIH/NAEPP Expert Panel Report 3 (4)
- The Global Initiative for Asthma (GINA) 2008 guidelines
- Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e (5)
Moral of the story, you may have halted an exacerbation, but be a doctor and treat the underlying disease! And as a bonus, you will have one less patient crowding the asthma room next week.
*Extra Controller Medication Tips: If your patient is already on an inhaled corticosteroid, add a long-acting beta agonist (like formoterol or salmeterol) or get fancy and start them on a combined ICS-LABA inhaler twice daily (1).
Other important check points before you send that person home:
Check Compliance and Inhaler Technique.
Poor technique is associated with poor disease control, poor adherence if therapeutic benefit not experienced, more hospital visits and increased resource utilization (7).
Check out a short and sweet YouTube Video on: How to use an Inhaler.
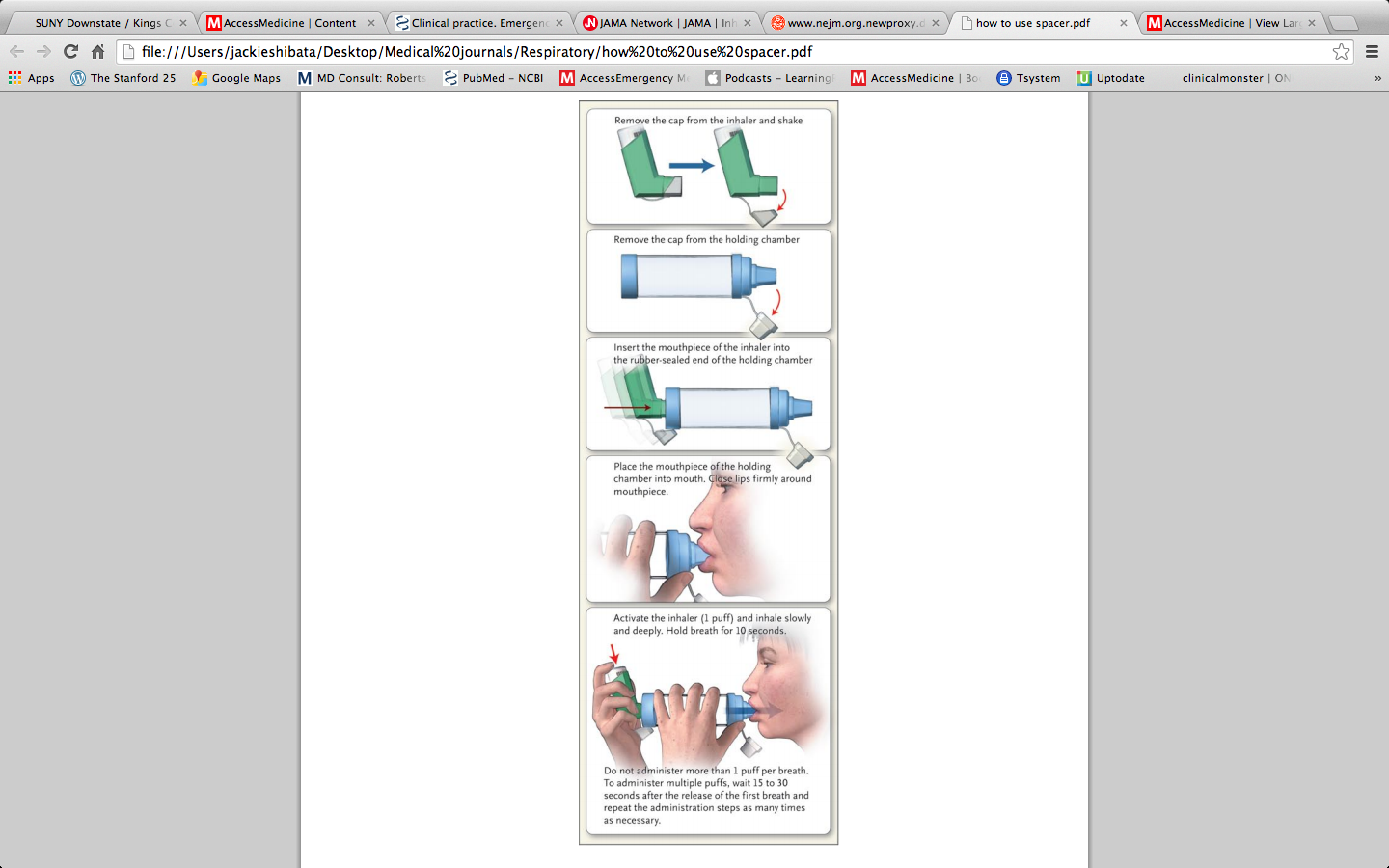
See how to use a spacer device from the NEJM (2):
Avoid Triggers and Quit Smoking!!
Tell them to avoid their triggers:
- Seasonal allergies? Second generation anti-histamines like Claritin and Zyrtec have been shown to reduce ED visits for asthma (3).
- Exercise-induced? Tell them to pre-treat with albuterol before they run.
- For the love of all the things, encourage them to quit smoking:
- 20% of asthmatics smoke. Smoking asthmatics have more severe disease, more hospital admissions, faster decline in lung function and a higher risk of death compared to non-smokers (1). Smoking also disrupts anti-inflammatory effects of asthma medications making them less effective. Cessation has been shown to improve lung function and steroid resistance (1).
*Note that they may have a temporary worsening of asthma immediately following smoking cessation.
But how can we get them to quit?!
Kanis et al. found that parents who perceived smoking as a risk to their child’s health were more likely to have a high motivation to quit smoking (8).
A recent systematic review of various smoking cessation interventions in the ED revealed only 2 studies had significant results; both used motivational interviewing and follow-up phone calls (9). Motivational interviewing is fascinating and a VERY effective communication skill that we should all learn to help patients see the error in their way, or as this video calls it, it’s a Jedi Mind Trick.
Check out this sample cartoon on smoking cessation using the 5 R’s of quitting (Relevance, Risk, Rewards, Roadblocks, Repetition):
Or if you prefer reading, this website lays out a brief intervention that you can add to your practice:
http://mdquit.org/cessation-programs/brief-interventions-5
Bottome line: Smoking is bad for asthma, but the best way for us ED docs to intervene is still unknown, but motivational interviewing (MI) may be effective.
Follow Up
Ok you’re right a lot of this is pretty IM-ish. Therefore, send them for follow-up with either an asthma specialist or a PMD. Sin et al. found that follow-up within 30 days of an asthma related ED visit was associated with a reduced 90-day re-admission rate (3).
In Conclusion (after your patient is back to breathing and talking):
Step 1. Ask about triggers – recommend avoidance and briefly talk about their motivation to quit smoking.
Step 2. Technique – Make sure they’re using their inhaler correctly.
Step 3. Educate them on controller and rescue medications
*Make sure they know:
– to keep the rescue medication with them at all times.
– use the controller medication everyday regardless of symptoms.
– re-iterate that the controller medication will not help them in acute exacerbation.
– don’t be afraid to start that inhaled corticosteroid!
Step 4. Set them up with follow up.
*Many of these young asthmatics do not have PMDs.
… Someone’s gotta prescribe that awesome controller med you started.
Step 5. Prescribe refills – for albuterol and their other controller meds.
*The controllers are necessary to prevent relapse after the oral steroids are completed.
Step 6. Enjoy a quieter asthma room next week and feel good, you saved another one!
References:
- Barnes PJ. Chapter 254. Asthma. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson J, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 18e. New York, NY: McGraw-Hill; 2012.
- Lazarus SC: Emergency treatment of asthma. N Engl J Med 363:755, 2010 [PubMed: 20818877]
- Rowe BH, Bota GW, Fabris L, Therrien SA,Milner RA, Jacono J. Inhaled budesonide in addition to oral corticosteroids to prevent asthma relapse following discharge from the emergency department: a randomized controlled trial. JAMA1999;281:2119-2126
- National Asthma Education and Prevention Program, Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.Publication No. 08-4051. Bethesda, MD, National Institutes of Health, 2007.
- Cydulka RK. Chapter 72. Acute Asthma in Adults. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011.
- Camp et al. ED visits for Children with Acute Asthma: discharge instructions, parental plans, and a follow-through of care – a prospective study. CJEM 2014 Nov. Vol 16:6.
- Crane et al. Inhaler device technique can be improved in older adults through tailored education: findings from a RCT. NPJ Prim Care Resp Med. 2014 Sep 4:24: 14034.
- Kanis et al. Motivation to quit smoking in parental smokers in the pediatric emergency department. Pediatr Emerg Care 2014 Aug: 30(8)546-51.
- Pelletier et al. A systematic review of smoking cessation interventions in the emergency setting. Am J Emerg Med 2014 Jul 32(7) 713-24.
jshibata
- Resident Editor-in-chief of blog.clinicalmonster.com
- Blog author of kchemimage.wordpress.com/category/clinical-radiographs/
- Co-author of the Resident Journal Review for AAEM’s Common Sense newsletter.
- EM/IM Resident at Kings County Hospital
Latest posts by jshibata (see all)
- Tox Craze - July 30, 2015
- PE or not PE, that is the question… - July 29, 2015
- Right on Target: A Petite Peds Post - July 6, 2015
- ARVD/C - June 18, 2015
- A dose of primary care for hyperglycemia in the ED: optimizing the discharge. - May 5, 2015
2 comments for “You think you know asthma?”