
Racial disparities in medical care exist. Did you know that you are more likely to receive a cardiac catheterization when you have chest pain with EKG abnormalities if you are white?[1] Or that if you are a minority, you are less likely to receive appropriate analgesia for long-bone fractures, cancer, and post-operative pain?[2]
Pain is the number one reason patients come to the Emergency Department, accounting for approximately 42% of all visits[3], yet physicians often undertreat pain, especially in minority patients, despite the fact that undertreating pain causes patient dissatisfaction, decreases patient cooperation, increases potentially preventable bounce backs to the ED, and delays return of full health and function.[4]
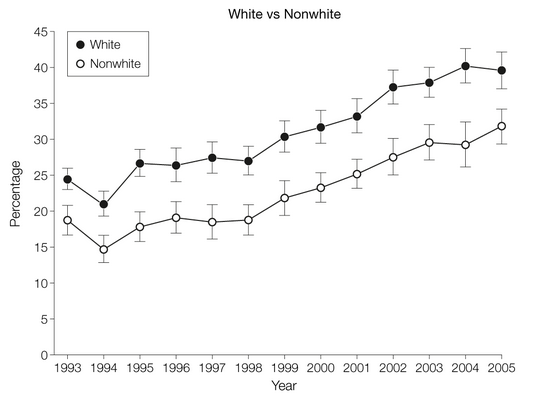
Opioid prescribing is increasing in all race/ethnic groups (P.001). National Hospital Ambulatory Medical Care Survey 1993-2005.
In 2008, a large study was published analyzing ethnic disparities in opioid prescribing for patients presenting to the ED with pain. 156,729 pain-related ED visits were analyzed between 1993-2005. Over the 13-year study period, whites were more likely to receive an opiate for pain-related visits than any other race: Whites (31%), Blacks (23%), Hispanics (24%). Disparities in opioid prescribing persisted regardless of pain severity, type of pain (IE abdominal pain, headache, etc), number of recurrent visits for similar complaint, and in 2 specific “painful” diagnoses: long-bone fractures and nephrolithiasis. In fact, as the pain severity increased, so did the disparity between opioids prescribed for whites and nonwhites (P=.01). The one exception to this trend was for patients with sickle cell disease, who were often treated with opioids.[5]
In 1999, Congress requested that the Institute of Medicine (IOM) explore disparities in healthcare and in 2002 they released the powerful study, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care” that identified three provider mechanisms that may perpetuate health care disparities for minorities: (1) bias or prejudice (2) clinical uncertainty (3) stereotypes held by the provider about minorities.[6]
As an academic institution, not only do we care for a diverse patient population, engage in medical research, and train future healthcare professionals; we represent the innovators and leaders of the medical community. Dr. Joseph Betancourt of the Disparities Solution Center urges academic institutions such as ours to act on the IOM’s recommendations by increasing awareness of disparities through collecting and reporting data by patients’ race/ethnicity, grand rounds, teaching how stereotypes may affect clinical decision-making in our medical education, using evidence-based treatment guidelines, using more professional interpreter services, and increasing the proportion of underrepresented minorities in the health care field.[7]
Congratulations, reading this blog post is one way of increasing your racial disparities in medicine awareness!
-Wendy Chan, MD
- Schulman, Kevin A., Jesse A. Berlin, William Harless, Jon F. Kerner, Shyrl Sistrunk, Bernard J. Gersh, Ross Dubé, Christopher K. Taleghani, Jennifer E. Burke, Sankey Williams, John M. Eisenberg, William Ayers, and José J. Escarce. “The Effect of Race and Sex on Physicians’ Recommendations for Cardiac Catheterization.” New England Journal of Medicine340.8 (1999): 618-26. Web.
- Rodriguez, Fatima, MD, MPH, and Alexander Green, MD, MPH. “Implicit and Explicit Ethnic Bias Among Physicians.” Culture, Brain, and Analgesia: Understanding and Managing Pain in Diverse Populations. Oxford: Oxford UP, 2013. 159-67. Print.
- Cordell, William H., Kelly K. Keene, Beverly K. Giles, James B. Jones, James H. Jones, and Edward J. Brizendine. “The High Prevalence of Pain in Emergency Medical Care.” The American Journal of Emergency Medicine20.3 (2002): 165-69. Web.
- Todd, Knox, MD, MPH, and Pletcher, Mark MD, MPH. “Ethnic Disparities in Emergency Department Pain Management” Culture, Brain, and Analgesia: Understanding and Managing Pain in Diverse Populations. Oxford: Oxford UP, 2013. 168-78. Print.
- Pletcher, M. J., S. G. Kertesz, M. A. Kohn, and R. Gonzales. “Trends in Opioid Prescribing by Race/Ethnicity for Patients Seeking Care in US Emergency Departments.” JAMA: The Journal of the American Medical Association299.1 (2008): 70-78. Web.
- Smedley, Brian, Adrienne Stith, and Alan Nelson. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Rep. no. ISBN: 978-0-309-08532-8. N.p.: National Academies, 2003. Print
- Betancourt, Joseph R. “Eliminating Racial and Ethnic Disparities in Health Care: What Is the Role of Academic Medicine?” Academic Medicine81.9 (2006): 788-92. Web.
wendyrollerblades
Latest posts by wendyrollerblades (see all)
- EM-CCM Hematology 7/22/2015:Treating DIC - July 27, 2015
- Critical Care: Recent Trials in Sepsis - May 1, 2015
- TASER Conducted Electrical Weapon Injuries - March 9, 2015
- Racially Biased Pain Control in the ED - December 15, 2014
- Cyra Whaa?!: Cautionary Tales About ER Folks Who Didn’t Use Skilled Translators - September 22, 2014