
47 year-old female with past medical history of depression and supraventricular tachycardia, brought in by EMS with altered mental status and found with empty pill bottles nearby.
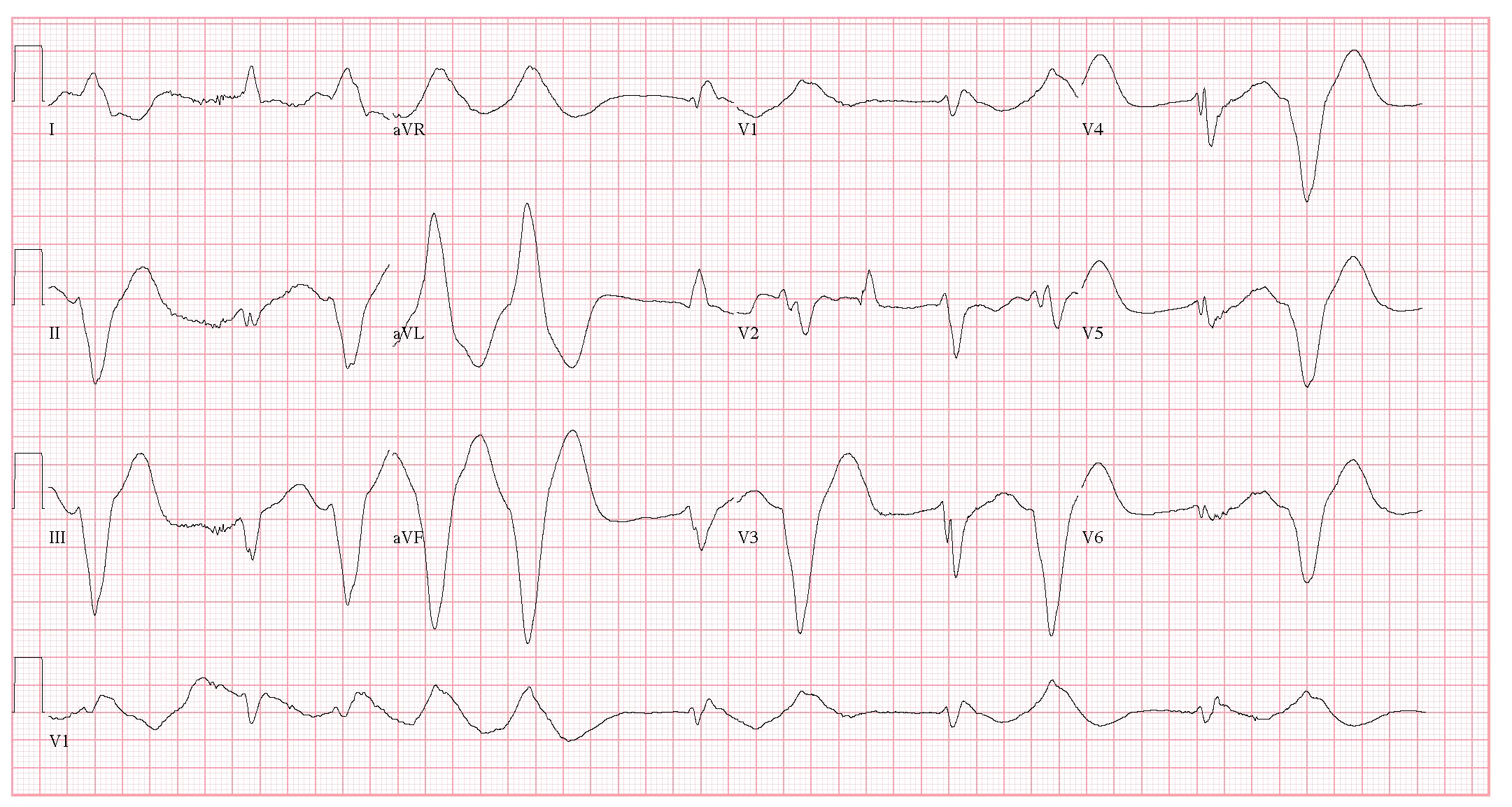
What is the interpretation of this ECG?
What likely happened to this patient?
How do you treat it?
Best answer by December 19, 2014 at noon will win!
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

eabram
Latest posts by eabram (see all)
- Rhythm Nation May 2015 Answer! - June 1, 2015
- Rhythm Nation May 2015 - May 10, 2015
- Rhythm Nation April 2015 – Answer! - April 20, 2015
- Rhythm Nation April 2015 - April 13, 2015
- Rhythm Nation March 2015 – Answer! - March 31, 2015
3 comments for “Rhythm Nation December 2014”