
28 year old male presents to the ED complaining of severe coughing, shortness of breath and chest pain. Denies fever or chills. But persistently complains of the severe coughing during history taking. States that only the last two days he has had the chest pain and shortness of breath, which brought him to the ED.
You get a CXR:
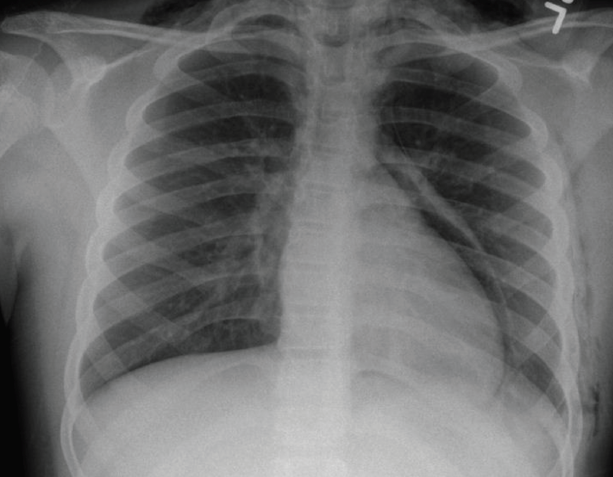
Please provide a complete read. What would you do for the patient?
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

jwang
Latest posts by jwang (see all)
- Xray Vision Answer - May 24, 2015
- Xray Vision: My Arm Looks Funny…. - May 16, 2015
- Xray Vision: Limping Answer - April 27, 2015
- Xray Vision: Limping - April 17, 2015
- Xray Vision: Answer - March 27, 2015
1 comment for “Xray Vision: Air Air Everywhere”