
Here’s the image again:
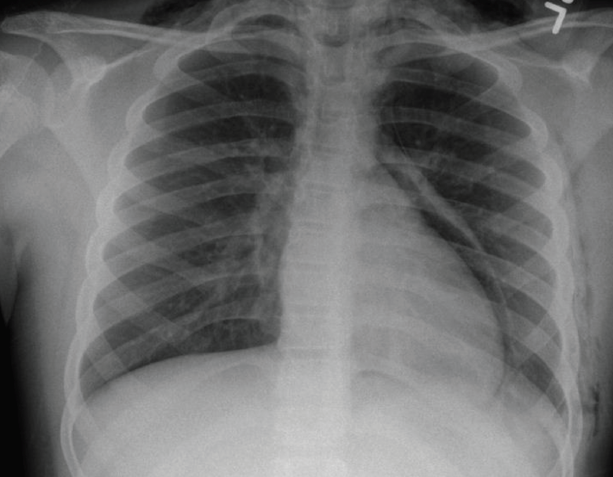
Congrats to Dr. Yohannes! The official read was: “pneumomediastinum and subcutaneous emphysema along the left chest wall and bilateral neck.”
Pneumomediastinum
Definition: free air within the mediastinum, which originates from the airways or the alveolar space. Despite how scary it appears, it rarely leads to severe complications, though there are case reports of pneumomediastinum leading to tension pneumomedistinum! Elevated mediastinal pressure can actually diminish cardiac output through direct cardiac compression and/or reduced venous return.
Pathophysiology: alveolar rupture leading to air dissection along the bronchovascular sheath, which causes free air to reach the mediastinum. The free air can also dissect into the submandibular space, the retropharyngeal space or the vascular sheaths within the neck as the mediastinum communicates with these structures.
CausesElevated pulmonary (alveolar) pressures: forceful coughing, crying or shouting. Vomiting, defecation, Valsalva maneuver, and illicit drug use (cocaine, inhalants) can also increase pulmonary alveolar pressure.
Respiratory Illness: obstructive lung disease (asthma, COPD, bronchiolitis) or intubated or mechanically ventilated patients.
Blunt or Penetrating injury
Presentation
Chest pain
Dyspnea
Fever – low grade fever and is associated with cytokine release.
Dysphonia
Throat pain
Physical exam findings
Workup
CXR – usually reveals air within mediastinal space.
CT chest – can diagnose pneumomediastinum not seen on cxr and can provide additional diagnostic information about the presence of coexisting illness, such as perforated esophagus.
You can consider ABG to evaluate respiratory distress in patients with respiratory distress. Cardiac enzymes if presentation of chest pain has unclear etiology. Consider urine or blood toxicology if indicated.
Treatment
Most pneumomediastinum are asymptomatic and resolve on their own.
Mechanical ventilation: If necessary, use lower pressures and tidal volumes.
Observation: close monitoring for possible serious complications with pulse oximetry and/or cardiorespiratory monitors).
Avoid strenuous physical activity, force expiratory maneuvers: spirometry or pulmonary function test.
Take home point:
Pneumomediastinum is almost always benign. Morbidity or mortality is associated with underlying condition, so treat the underlying condition.
jwang
Latest posts by jwang (see all)
- Xray Vision Answer - May 24, 2015
- Xray Vision: My Arm Looks Funny…. - May 16, 2015
- Xray Vision: Limping Answer - April 27, 2015
- Xray Vision: Limping - April 17, 2015
- Xray Vision: Answer - March 27, 2015