
Congratulations to both responders who weren’t fooled for a second! This month’s winner is Dr. Nico Grundmann with honorable mention to Dr. Brenda Oiyemhonlan!
Onto the ECG
A bifascicular block with a possible (i.e. incomplete) underlying trifascicular block. What makes it “possible” instead of definite? Clear evidence of conduction blocks at two specific locations, the right bundle branch and left anterior fascicle, with a 1st degree AV block of unknown location. The interpretation of this ECG should be broken down step by step and approached systematically as Drs. Grundmann and Oiyemhonlan have demonstrated.
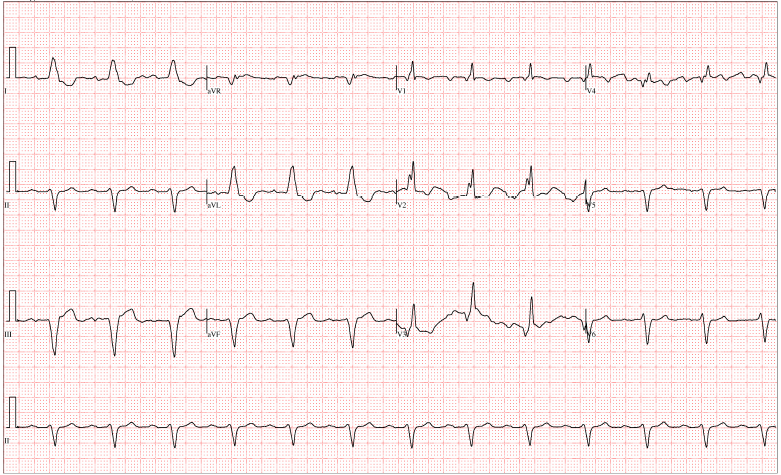
1st degree AV block w/ RBBB & LAFB and inferior q-waves
The Breakdown
The clear P-waves in lead II show a PR interval >200ms (longer than one big box), therefore a 1st degree AV block is also present.
There is also a right bundle branch block due to the QRS >120ms (or larger than three small boxes),with classic RBBB pattern:
- RR’ in right sided precordial leads, most prominent in V2 here
- Slurred S-wave in the left sided leads, usually seen in V5-V6 but most prominent in I and aVL here
Lastly, a left anterior fascicular block is here as defined by left axis deviation (the QRS has a negative deflection in both aVR and lead II), AND a qR (small/absent q-wave, tall R-wave) in leads I, aVL AND an rS (small/absent r-wave, deep S-wave) in leads II, III, aVF. Any time the axis is deviated, always look at the size/magnitude ratio of waves within the QRS complex to evaluate for a fascicular block. Keep in mind, there are other causes of left or right axis deviation.
Now, let’s put all of this together…
There are essentially 3 fascicles which conduct to the ventricles. The left bundle branch gives off two of them, the left anterior fascicle (LAF) & left posterior fascicle. The right bundle branch makes up the 3rd fascicle. This ECG shows a RBBB and a LAFB, meeting criteria for a bifascicular block… While there are “essentially 3 fascicles”, technically there is a 4th fascicle that comes off the left bundle branch, the septal fascicle, but it’s the forgotten step-child of ECGs that no one knows what to do with, so everyone just ignores it. And so will we from this point on.
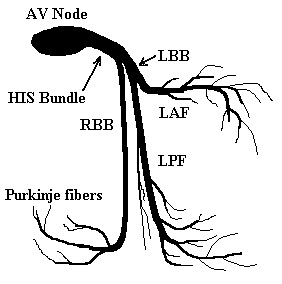
Image taken from Life in The Fast Lane at http://lifeinthefastlane.com/ecg-library/trifascicular-block
A 1st degree block does not completely block conduction (such as 2nd or 3rd degree block), it merely slows down conduction to the ventricles. Though a 1st degree block can occur anywhere from the SA node to the ventricles, they are most commonly located at the AV node. The location of the 1st degree block influences the danger the trifascicular block poses. For example if it lies in the left posterior fascicle, in the presence of a RBBB and LAFB this would then meet criteria for trifascicular block (because all three fascicles are inhibited independently). If the 1st degree block is located higher up, say at the AV node or anywhere more proximal, then it would affect all three fascicles equally which is much less concerning.
Trifascicular block can spiral into complete heart block (hint: not good). So… it’s very important to identify trifascicular block early!
The different types of trifascicular block are:
- Alternating bundle branch blocks on ECGs recorded at different times in the same patient
- Fixed RBBB + alternating fascicular blocks (Hint: the axis will be deviated in opposite directions with LAFB and LPFB).
- RBBB or LBBB + 2nd degree type II block, indicating a fixed block in one bundle branch and an intermittent block in the other
*Note: these rhythms show evidence of disease in all three fascicles.
Possible or incomplete trifascicular block are:
- Bifascicular block + 1st degree or 2nd degree type I block
- Complete AV block with ventricular escape (sounds crazy, I know). Complete heart block in a patient with known bifascicular block is almost certainly due to disease of the 3rd fascicle (i.e. trifascicular block). However, technically the block can occur proximal to the bundle branches, in which the bundle of His should take over as the pacemaker, but if this does not take place then a ventricular escape rhythm is the result.
*Note: these rhythms have evidence of bifascicular disease, with a 3rd block occurring at an unknown location.
Management
Since our patient presented in CHF exacerbation, the initial resuscitation management of IV/O2/monitor, ASA, preload reduction, afterload reduction, +/- noninvasive positive airway pressure, and eventual diuresis.
After seeing this ECG – he should also get pacer pads placed on him immediately.
If this possible/incomplete trifascicular block was new, a cardiology consult should be placed as the most concerning cause of a new 1st degree AV block in this specific patient would be inferior wall ischemia.
Lastly, if this were definite trifascicular block this would be a Class 1 indication for a permanent pacemaker. In the event of severe bradycardia with a ventricular escape rhythm, management would be discontinuing all AV nodal blocking agents (i.e. beta-blockers, ca-channel blockers, digoxin) and transcutaneous pacing until a transvenous pacer can be placed, ultimately followed by a permanent pacemaker.
By Dr. Yonatan Yohannes, Dr. Elizabeth Abram, and Dr. Jennifer Martindale. Editing by Dr. Andy Grock.
References:
Martidale, J. L. & Brown, D. F. M. (2012). Rapid Interpretation of ECGs in Emergency Medicine: A Visual Guide. Philadelphia, PA: Lippincott Williams & Wilkins.
Hayes, D. L. Indications for permanent cardiac pacing. Up To Date 2014. Uptodate.com.
Burns, E. (2014). Triafascicular Block. Life in the Fast Lane. Retrieved from http://lifeinthefastlane.com/ecg-library/trifascicular-block/.
Yonatan
Latest posts by Yonatan (see all)
- Morning Report: 6/29/2015 - June 29, 2015
- Rhythm Nation June 2015 – Answer! - June 20, 2015
- Rhythm Nation June 2015 - June 13, 2015
- Rhythm Nation January 2015 Answer! - January 18, 2015
- Rhythm Nation January 2015 - January 9, 2015