
Case Recap: Old lady with hypotension, tachycardia and JVD…
I think we all agree that this person is sick. Prior to pondering the wide differential do the Basics: 2 Large Bore IVs, O2 NC vs NRB, Monitor, assess airway
My Top Three Differential Diagnoses
1. Cardiac Tamponade
2. Massive PE
3. Inferior Wall MI with Cardiogenic Shock
Do you want to give fluids?
Tricky question! IV fluids helps BP in PE and Tamponade…but can be a poor idea in cardiogenic shock. Remember, in cardiogenic shock the heart can’t pump the fluid out leading to decreased venous return as demonstrated by JVD. Fluids in cardiogenic shock are generally a bad idea as they increase an already overloaded pre-load. Since her lungs are clear iIn this case, you can give a “100ml to 250ml bolus” [1] and reassess the patient for improved BP and the development of rales.
Once Basics Are Done
ECG and Echo. Yes, labs/cxr are also needed, but they won’t help you differentiate between the above three in a timely fashion.
Her Echo may have looked like this…
Apical 4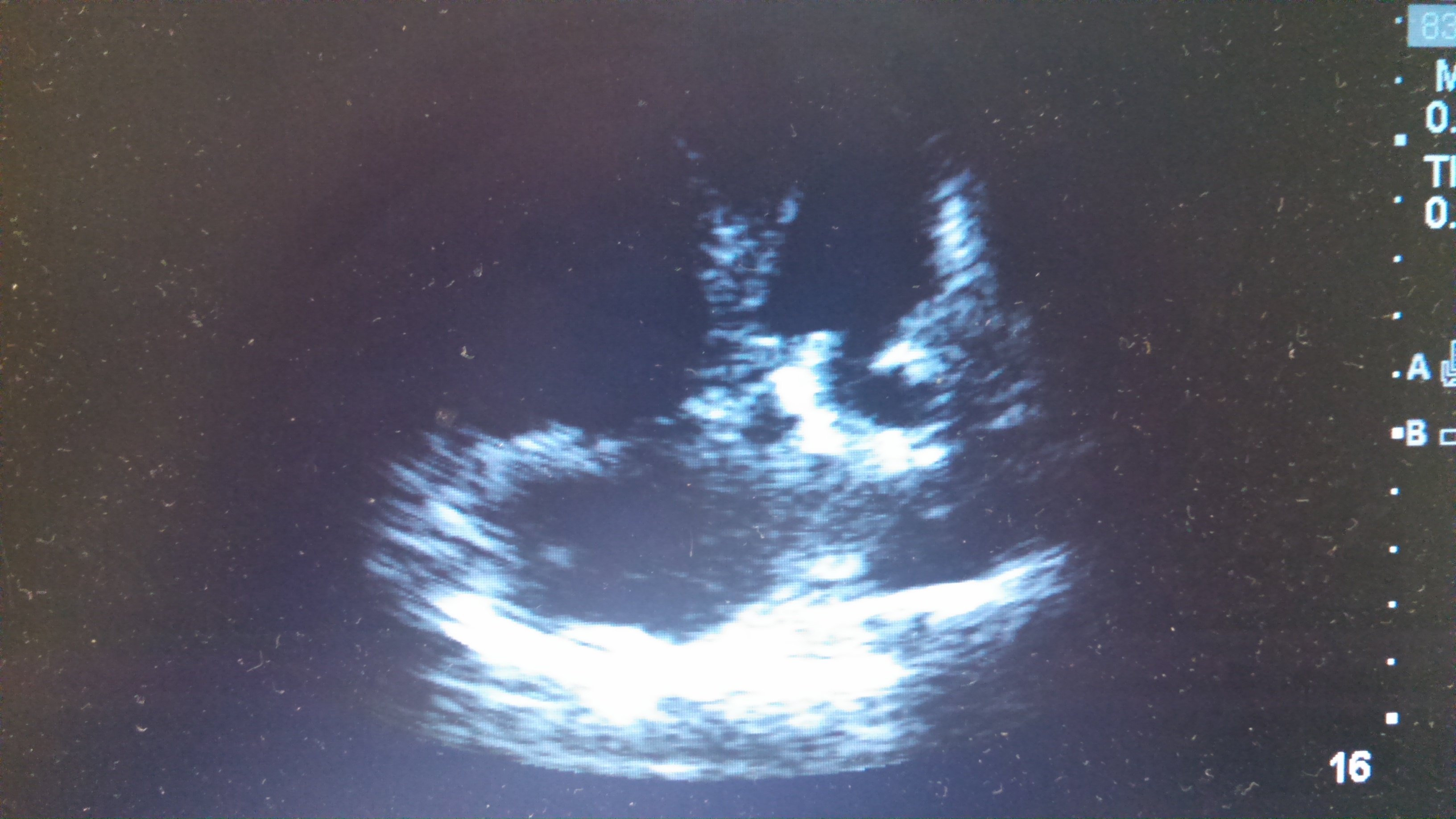
Parasternal Short
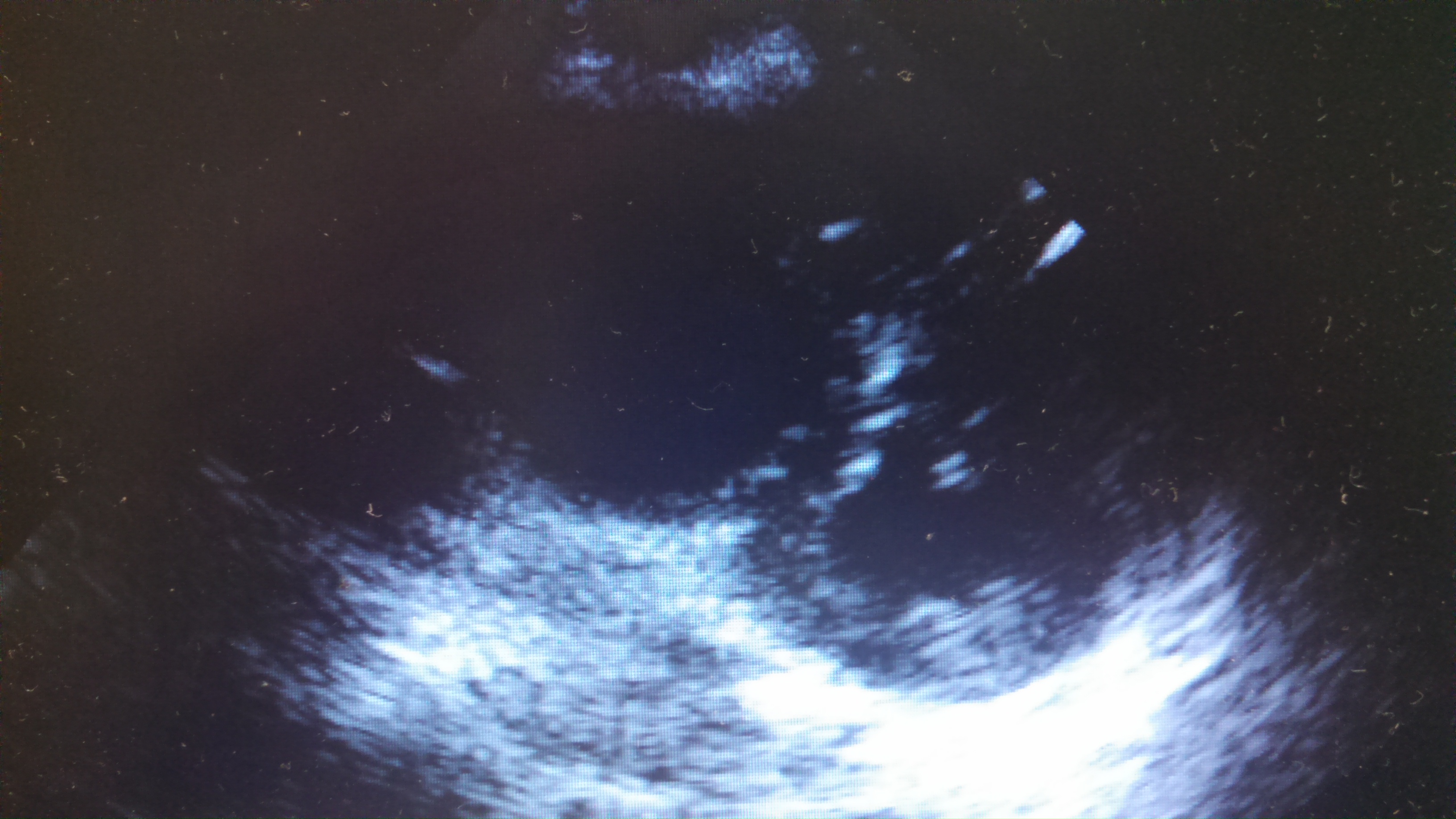
Parasternal Long
What findings are on these US images?
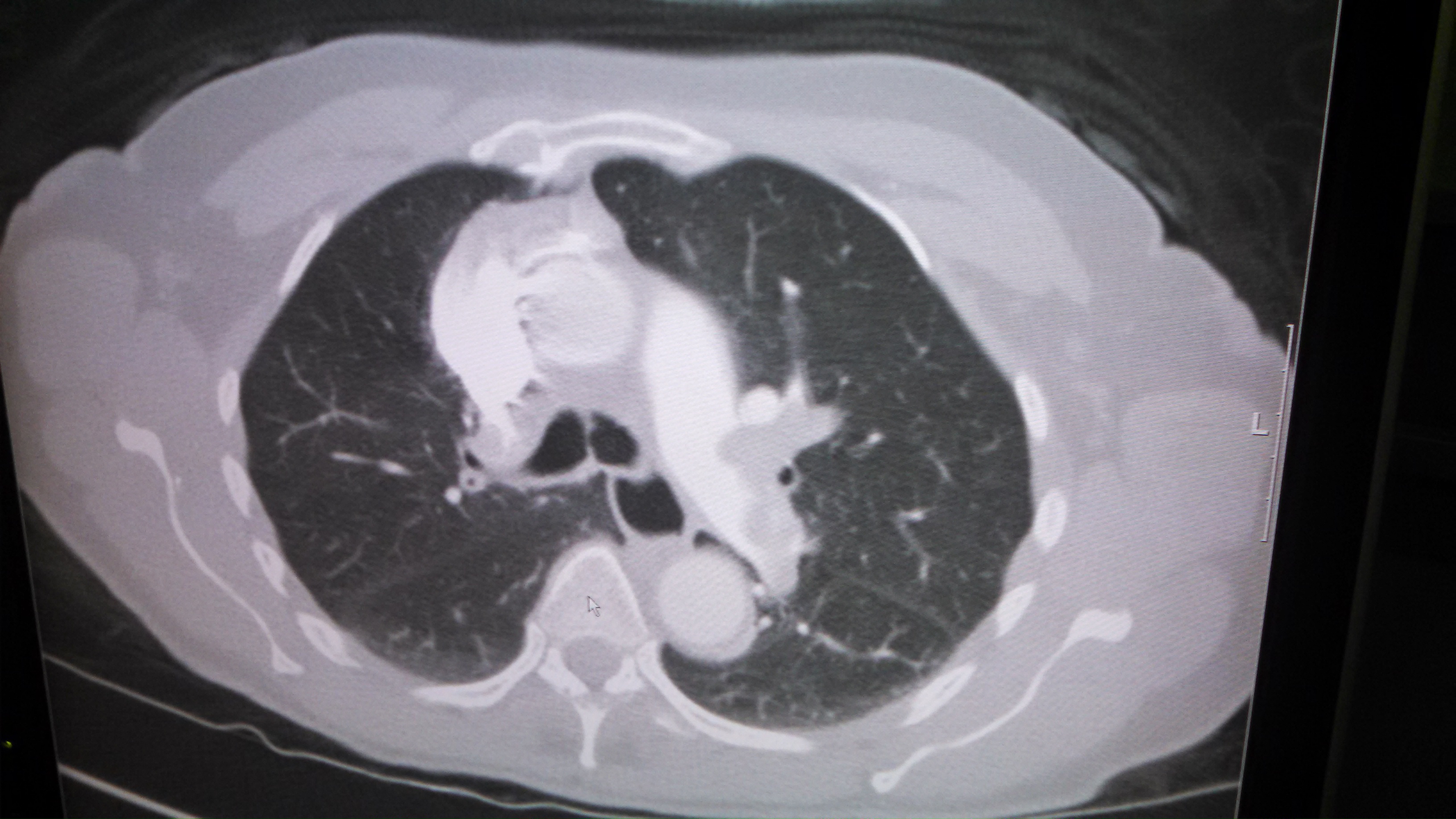
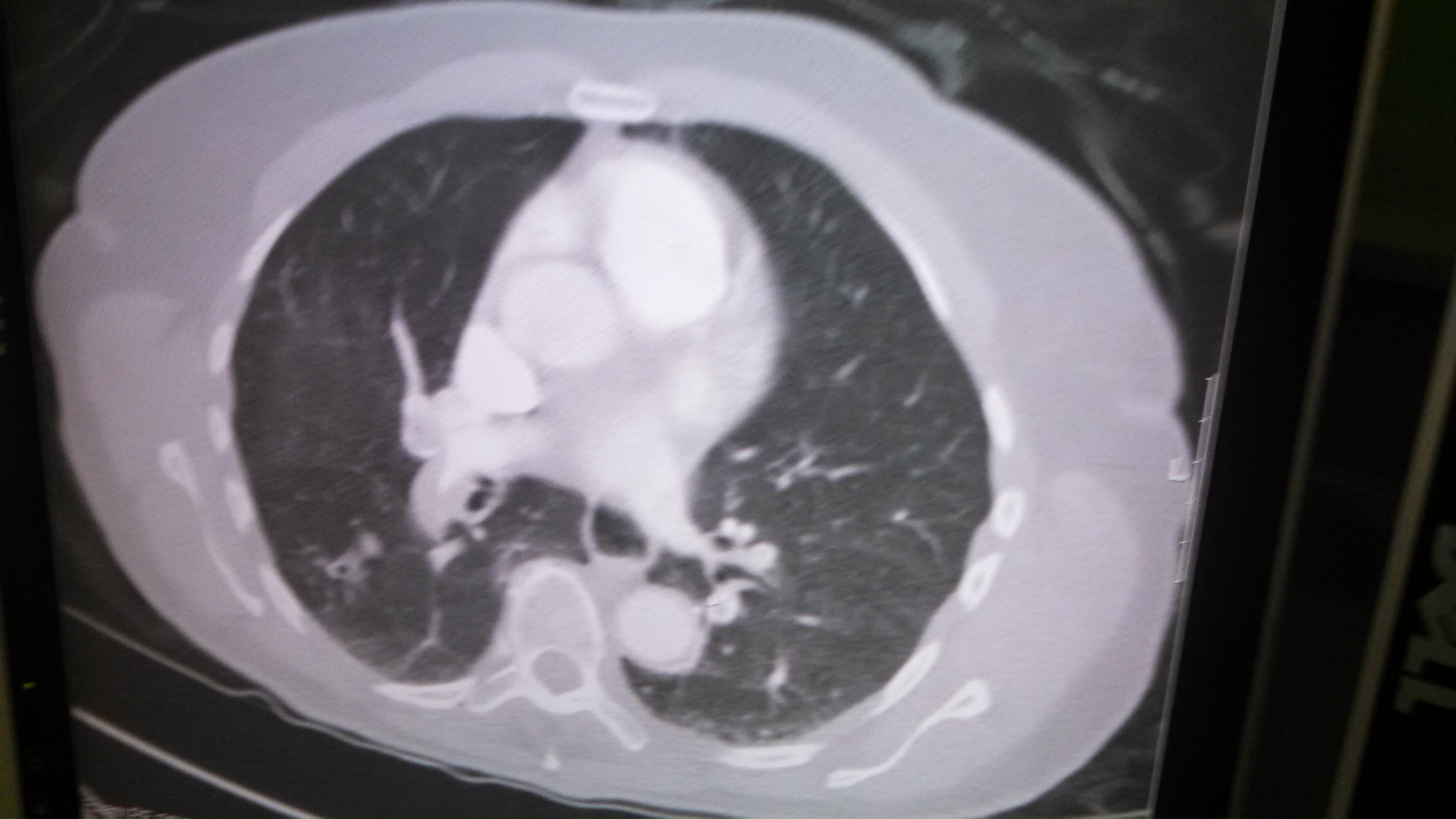
If the patient improves enough to get a CT...
Treatment?
By Dr. Andrew Grock
Special thanks to Dr. Ian deSouza.
References
[1] Tintinalli’s 7th ed.
andygrock
- Resident Editor In Chief of blog.clinicalmonster.com.
- Co-Founder and Co-Director of the ALiEM AIR Executive Board - Check it out here: http://www.aliem.com/aliem-approved-instructional-resources-air-series/
- Resident at Kings County Hospital
Latest posts by andygrock (see all)
- A Tox Mystery…. - May 26, 2015
- Of Course, US Only for Kidney Stones… - May 18, 2015
- Case of the Month 11: Answer - May 12, 2015
- Too Classic a Question to Be Bored Review - May 5, 2015
- Case of the Month 11: Presentation - May 1, 2015
3 comments for “Case #7, Answer”