
Happy New Year to All!
Now, back to business…
A 71 year-old male with past medical history of CAD and CHF (last known EF 10%) is sent by his PMD for progressive shortness of breath, dyspnea on exertion, and lower extremity edema.
Just as you sit down to finally catch up on notes, you are handed the ECG below.
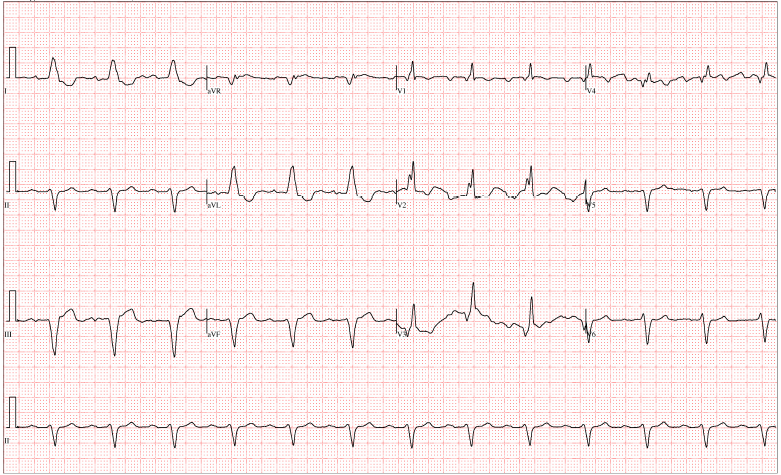
What is your interpretation of this ECG?
What type of conduction abnormality would you be most concerned for and why?
Briefly, how would you manage this patient in the Emergency Department?
Best response by 12pm on 1/16/15 wins!
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

Yonatan
Latest posts by Yonatan (see all)
- Morning Report: 6/29/2015 - June 29, 2015
- Rhythm Nation June 2015 – Answer! - June 20, 2015
- Rhythm Nation June 2015 - June 13, 2015
- Rhythm Nation January 2015 Answer! - January 18, 2015
- Rhythm Nation January 2015 - January 9, 2015
2 comments for “Rhythm Nation January 2015”