
EM-CCM Review: Renal
Presenter: Dr. Brenda Oiyemhonlan
Review by: Sally Bogoch
This block’s EM-CCM was a fantastic review of a commonly seen problem at its extreme. For the sake of brevity we will review:
- Renal failure associated metabolic derangements
- Indications for urgent dialysis
- Treatment of hyperkalemia- this is our bread and butter
- To bicarb or not to bicarb
- Not all troponinemia is caused by coronary artery disease.
The case: In a fictitious hospital in coastal USA, a 53-year-old male with a history of hypertension presents with shortness of breath. He recently travelled from Kenya, where he lives with his family. He reports having had leg swelling, shortness of breath and decreased exercise tolerance to just several steps at a time over the last three months. Physical examination is significant for moderate respiratory distress, tachypnea, hypertension, tachycardia, abdominal distension, bilateral pitting lower extremity edema, bilateral rales, JVD to the angle of the mandible and a loud S3 gallop. Long story long, the patient was ultimately found to be in renal failure, profoundly anemic, with significant electrolyte abnormalities (hyperkalemia, acidemia) and elevated troponin with obvious clinical signs of fluid overload from renal failure. Let’s discuss…
Metabolic derangements in renal failure:
- Erythropoietin is made in the kidneys. When the kidneys have failed, they make no erythropoietin. The result is a chronic anemia that can approach critical levels. Strategies to fix this include red blood cell transfusion in the acute setting and recombinant erythropoietin/synthetics to stimulate the bone marrow to produce red blood cells.
- Acidosis in renal failure is multifactorial. The kidneys are unable to appropriately exchange hydrogen ions for potassium in the distal collecting ducts of the nephron and are functionally unable to excrete acids (most often excreted as ammonium). As well, hyperkalemia stimulates the shift of potassium intracellularly in exchange for serum acids. Bicarbonate falls in an attempt to buffer the excess acids, metabolic acidosis ensues. The anion gap metabolic acidosis is usually caused by urea, the non-anion gap metabolic acidosis of renal disease is hyperchloremic.
- Vitamin D is the cofactor for calcium absorption in the gut, but not until it is hydroxylated in the kidney. When the kidney has failed, calcium is therefore not able to be absorbed. As well, the kidneys are not able to filter phosphate. The subsequent rise in serum phosphate inhibits PTH, thus decreasing serum calcium. This is mostly a non-EM issue, but the patient in this situation had profound hypocalcemia. Look for muscle spasm, Chvostek’s sign, Trousseau’s sign, and EKG changes (prolonged QT).
- This is the feared complication that causes dysrythmias. Potassium excretion by the kidneys is carefully related to glomerular filtration rate. When there is decreased delivery of sodium to the ascending loop of Henle and the distal collecting tubules, potassium is retained. This is due to the dysfunction of the renin-aldosterone mechanism which is impaired in renal failure as the kidney is unable to respond to hormonal changes, thus resulting in hyperkalemia.
- Read beyond the basics about sick patients in renal failure here: Joslin, J., & Ostermann, M. (2012). Care of the Critically Ill Emergency Department Patient with Acute Kidney Injury. Emergency Medicine International, 2012, 1-6. Retrieved February 5, 2015, from http://dx.doi.org/10.1155/2012/760623
Indications for Urgent Dialysis
Remember this simple mnemonic:
A Acidosis, pH generally <7.0
E Electrolyte abnormalities, specifically hyperkalemia in ESRD or AKI
I Ingestions of toxins removed by dialysis: lithium, salicylates, ethylene glycol, etc.
O Overload. Fluid overload as demonstrated by pulmonary edema and fluid retention.
U Uremia- more specifically, uremia causing encephalopathy and pericarditis/effusion.
****Acute Kidney Injury and RIFLE****: in 2002, the Acute Dialysis Quality Initiative put together a classification for ACUTE KIDNEY INJURY, classifying worsening renal function as being at Risk, having renal Injury, new renal Failure, Loss of renal function, and End stage renal disease. These RIFLE classifications are based on changes in GFR, creatinine and urinary output over a period of 4 weeks. Many patients have REVERSIBLE causes for their renal failure (obstruction from BPH, nephrotoxic drug, inflammatory illness/glomerulonephritis). For some patients, brief dialysis may be needed to remove potassium until there is return of renal function. A common, reversible cause of AKI is volume depletion. The treatment is intravenous hydration- this alone can increase renal blood flow, glomerular filtration, and promote kaluresis by restoring the normal physiology of the kidney.
Foley catheter placement is often recommended by nephrologists to confirm urine output and help diagnose the cause of AKI. AKI due to post-obstructive uropathy, most commonly by BPH, and placing a Foley catheter may be necessary to reverse AKI in this case. Such catheters are a common cause of nosocomial/iatrogenic infections and should be avoided if at all possible. Along with a true urinary obstruction, catheters may be useful in critically ill patients who need strict monitoring of urinary output as a measure of tissue perfusion.As an alternative to placing a Foley catheter for diagnostic purposes, physicians may use bedside sonography to assess for urine production (fluid-filled bladder) and obstructive causes of AKI (bladder distension +/- hydronephrosis).
Treatment of Hyperkalemia in renal failure: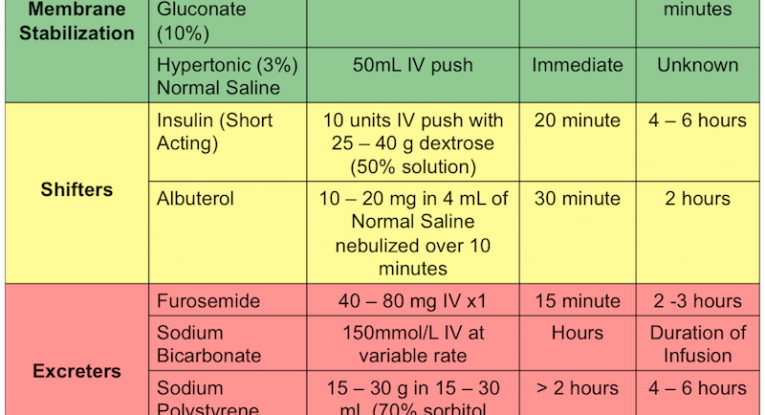
Bicarbonate: A Cochrane review (2009) shows mixed results with bicarbonate for hyperkalemia in renal failure when used in isolation. However, some of the studies showed benefit when used along with dextrose and insulin in the setting of acidosis with ESRD and hyperkalemia. The jury is still out in terms of benefit. It does not cause harm, however.
See Andy Grock’s awesome ALiEM post about bicarbonate here: http://www.aliem.com/bicarbonate-completely-useless/
Troponins.
Contrary to “popular belief”, troponin elevation in patients with renal failure is NOT due to reduced troponin clearance. Besides chronic renal injury as in this case, troponin may be elevated for anumber of reasons. The list includes, sepsis, strenuous exercise, rhabdomyelysis, heart failure, PE, not to mention myocardial infarction, heart surgery, pericarditis, myocarditis and cardiac catheterization.
- More here: Korff, S. (2006). Differential diagnosis of elevated troponins. Heart, (92), 987-993. Retrieved February 3, 2015, from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1860726/pdf/987.pdf
sbogoch
Latest posts by sbogoch (see all)
- EM-CCM Cardiology 3/18/2015:Care of the Post-Arrest Patient - April 9, 2015
- 3/10/2015: Bored of Cardiologists, not Cardiology - March 10, 2015
- Bored review: 3/3/2015 Looking Beyond the Injury - March 3, 2015
- Acute Kidney Injury- caring for the sick patient with new renal disease. - February 28, 2015
- Bored Review: 2/3/2015-EKG Changes that make you go hmmm. - February 3, 2015