
A 54-year-old female with diabetes, hypertension, end-stage renal disease on dialysis presents to the ED after “Snowmageddon” with a complaint of generalized weakness. She answers questions, but seems slightly confused. While awaiting for the initial vital signs, you feel her pulse and find that it is approximately 45. You place an IV while your colleague is putting the patient on the monitor. The PCA then hands you this EKG: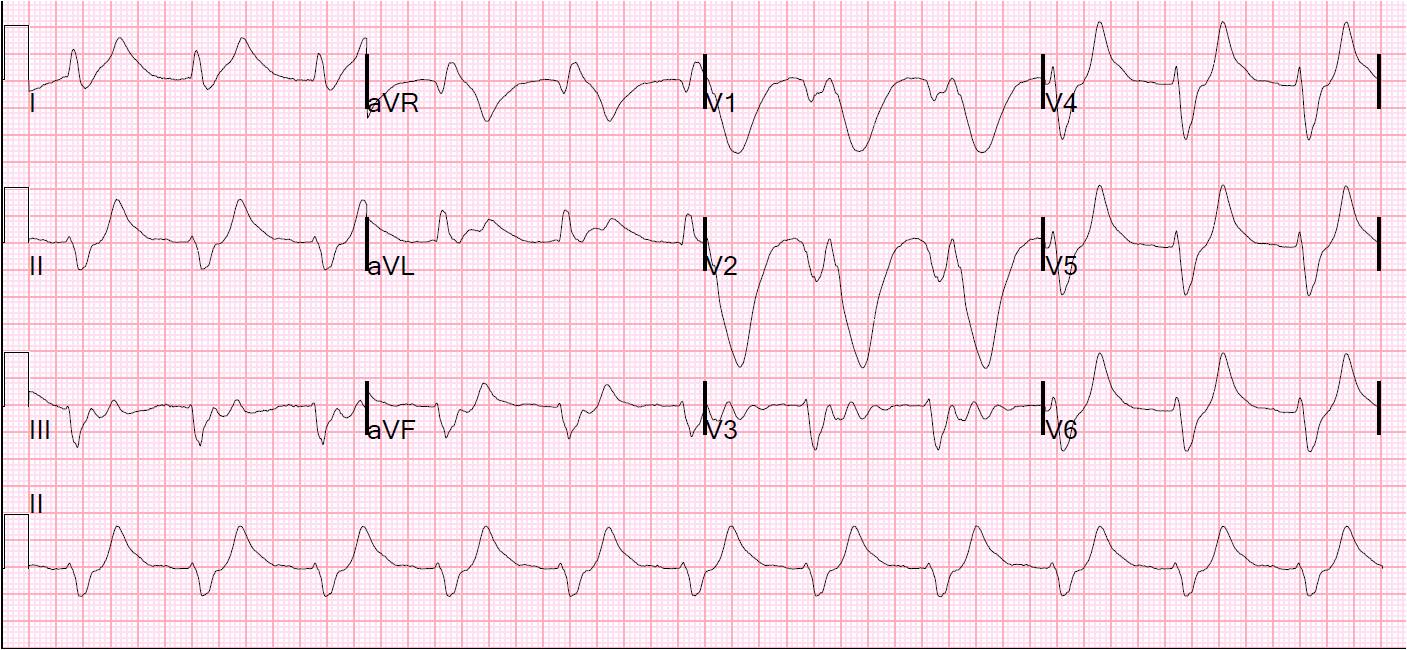
Your first response is:
a) ask to see an old EKG
b) soil yourself
c) call the renal fellow to arrange for dialysis
d) administer 1 gram of calcium gluconate IV push
answer1) stabilize the cardiac cell membranes
2) shift potassium into cells
3) excrete potassium from the body
Below is a chart demonstrating the onset and duration of the medications used for the above strategy. Just don’t give sodium polystyrene. It causes more harm than benefit and takes too long to work.
Ultimately, the best way for our above patient to excrete potassium is by hemodialysis- AFTER THEY HAVE BEEN STABILIZED!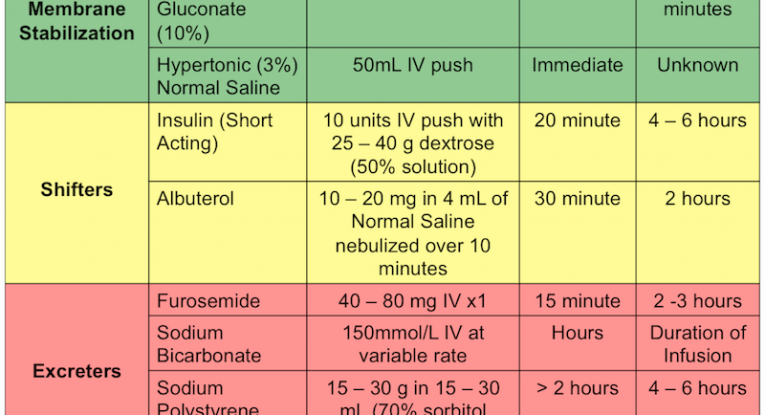
Rosen’s Emergency Medicine, 7th Edition.
By: Andy Grock and Sally Bogoch
sbogoch
Latest posts by sbogoch (see all)
- EM-CCM Cardiology 3/18/2015:Care of the Post-Arrest Patient - April 9, 2015
- 3/10/2015: Bored of Cardiologists, not Cardiology - March 10, 2015
- Bored review: 3/3/2015 Looking Beyond the Injury - March 3, 2015
- Acute Kidney Injury- caring for the sick patient with new renal disease. - February 28, 2015
- Bored Review: 2/3/2015-EKG Changes that make you go hmmm. - February 3, 2015
1 comment for “Bored Review: 2/3/2015-EKG Changes that make you go hmmm.”