
This month’s winner is the one and only ablumenberg, whose intimidatingly thorough answer frightened off all other contenders.
Recap
Older lady, many medical problems, here for epigastric discomfort now with acute decompensation as evidenced by her tachycardia and diaphoresis while in your imaginary ED.
This patient is clearly in shock. Let's start with a broad diff dx for shock as ablumenberg commented, this ECG is consistent with pericarditis. As you can see, there are generalized ST elevations, ST depressions in V1 and AVR, and PR depressions! Note there is no electrical alternans. ECG findings for pericarditis are well described in the textbook, BUT rarely progress as depicted. The 4 stages of are: 2. T wave flattening throughout 3. T wave inversions 4. Normal So what do you do about this? For this case, repeat ECG was rate 150, mildly irregular, with the same ST segments as seen previously. CXR was unchanged without air under the diaphragm. RUSH exam revealed no signs of right heart strain, no signs of pneumothorax, BUT a large pericardial effusion! Though there was no RV collapse or obvious atrial compression, there was a plethoric IVC! The treatment: pericardiocentesis or, if stable enough, an emergent pericardial window. So what are the signs of pericardial tamponade on ultrasound? By Dr. Andrew Grock References Life in the Fast Lane: http://lifeinthefastlane.com/ecg-library/basics/pericarditis/ Tintinally’s 7th ed EMCrit:http://emcrit.org/rush-exam/ Adam Goodman, Phillips Perera, Thomas Mailhot, and Diku Mandavia. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade. J Emerg Trauma Shock. 2012 Jan-Mar; 5(1): 72–75. Dina Seif, Phillips Perera, Thomas Mailhot, David Riley, and Diku Mandavia. Review Article Bedside Ultrasound in Resuscitation and the Rapid Ultrasound in Shock Protocol. Critical Care Research and Practice Volume 2012, Article ID 503254, 14 pages doi:10.1155/2012/503254 Ultrasound Podcast: http://www.ultrasoundpodcast.com/2013/11/pericardial-tamponade-learn-know-foamed/ 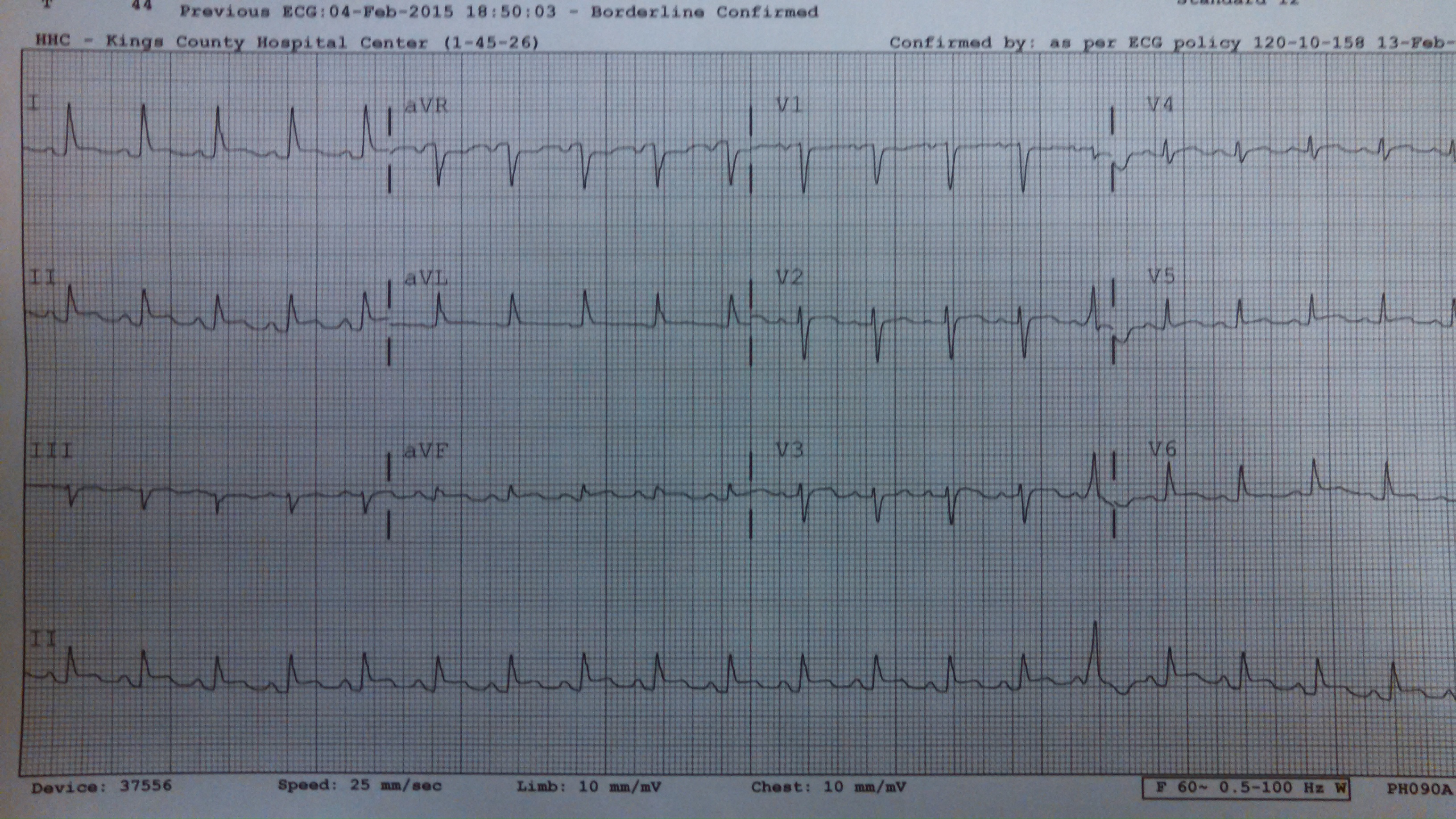
1. Generalized STE, PR depressions, ST depressions in AVR![]()
andygrock
![]()
Latest posts by andygrock (see all)