
A 58 year old woman with a long medical history – paroxysmal afib, not on anticoagulation, hyperthyroidism secondary to graves disease, and GERD who presents for the third ED visit in 1 month for epigastric pain. At her first visit, she improved after a GI cocktail, had a normal ECG/CXR/labs, and was discharged with next day stress test. She returned with the same complaint, improved with another GI cocktail, had a normal ECG and CXR, and was discharged.
You see her on her third visit with the same presentation. Her vital signs are as follows: HR 120, RR 18, BP 110/61, O2 sat 99%, Temp 98.3 oral.
She is complaining of the same epigastric pain radiating to the chest with mild nausea that she has had for months. Additionally, she has been taking 8-10 ibuprofen tabs a day. Her ECG is…
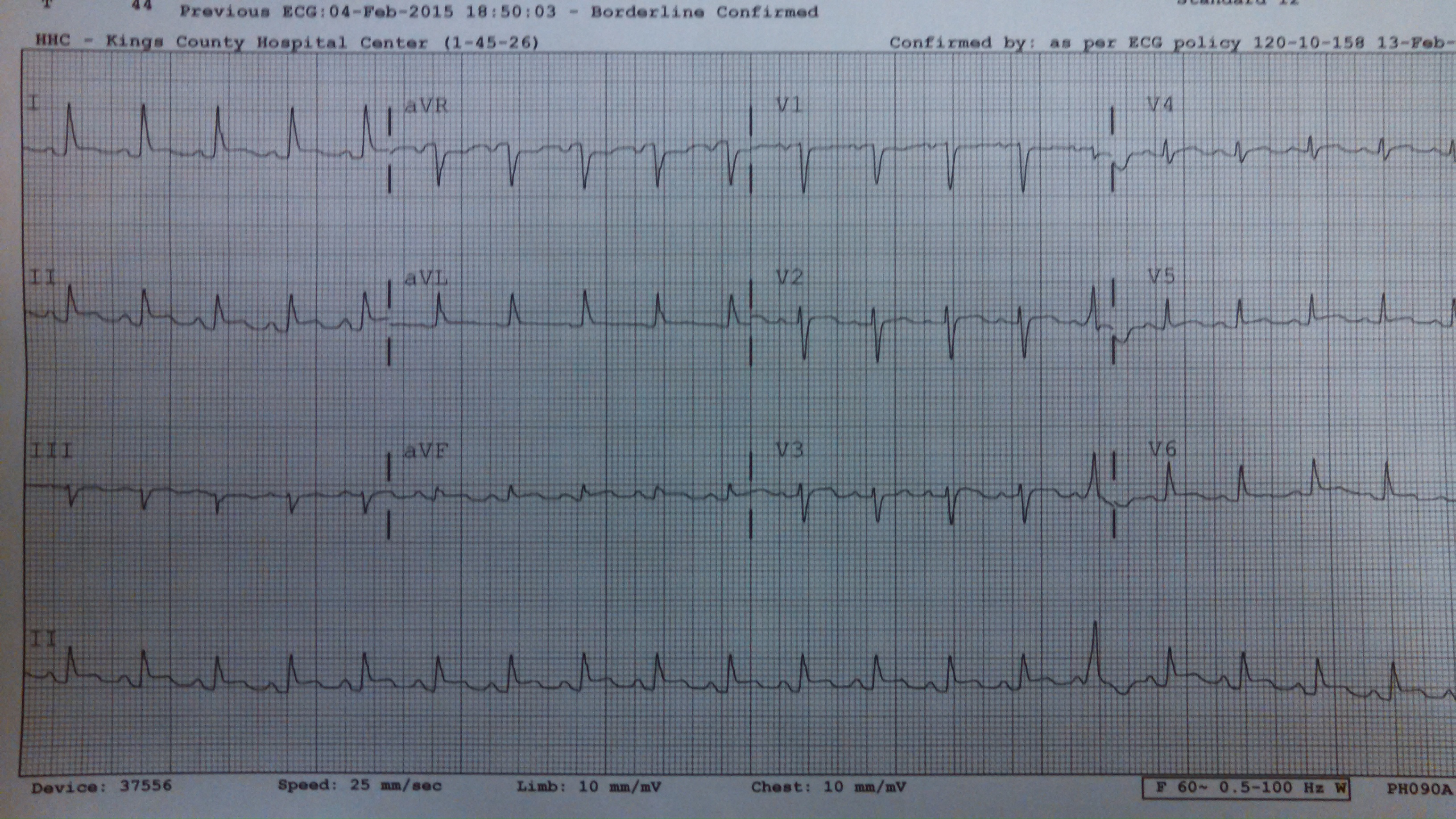
After a GI cocktail and normal labs including a negative troponin, you go back to reassess the patient. She is now complaining of L chest pain and appears mildly diaphoretic. You put her on the monitor and now her HR is in the 150s.
For this month’s big prize
1. Please list your top 3-5 diagnosis, the next diagnostic step or steps, and the ED management for ?
andygrock
- Resident Editor In Chief of blog.clinicalmonster.com.
- Co-Founder and Co-Director of the ALiEM AIR Executive Board - Check it out here: http://www.aliem.com/aliem-approved-instructional-resources-air-series/
- Resident at Kings County Hospital
Latest posts by andygrock (see all)
- A Tox Mystery…. - May 26, 2015
- Of Course, US Only for Kidney Stones… - May 18, 2015
- Case of the Month 11: Answer - May 12, 2015
- Too Classic a Question to Be Bored Review - May 5, 2015
- Case of the Month 11: Presentation - May 1, 2015
1 comment for “Case of the Month #9, Presentation”