
Kudos go to Dr. Bryan Jarrett for an excellent interpretation!
Much discussion was had over this ECG.
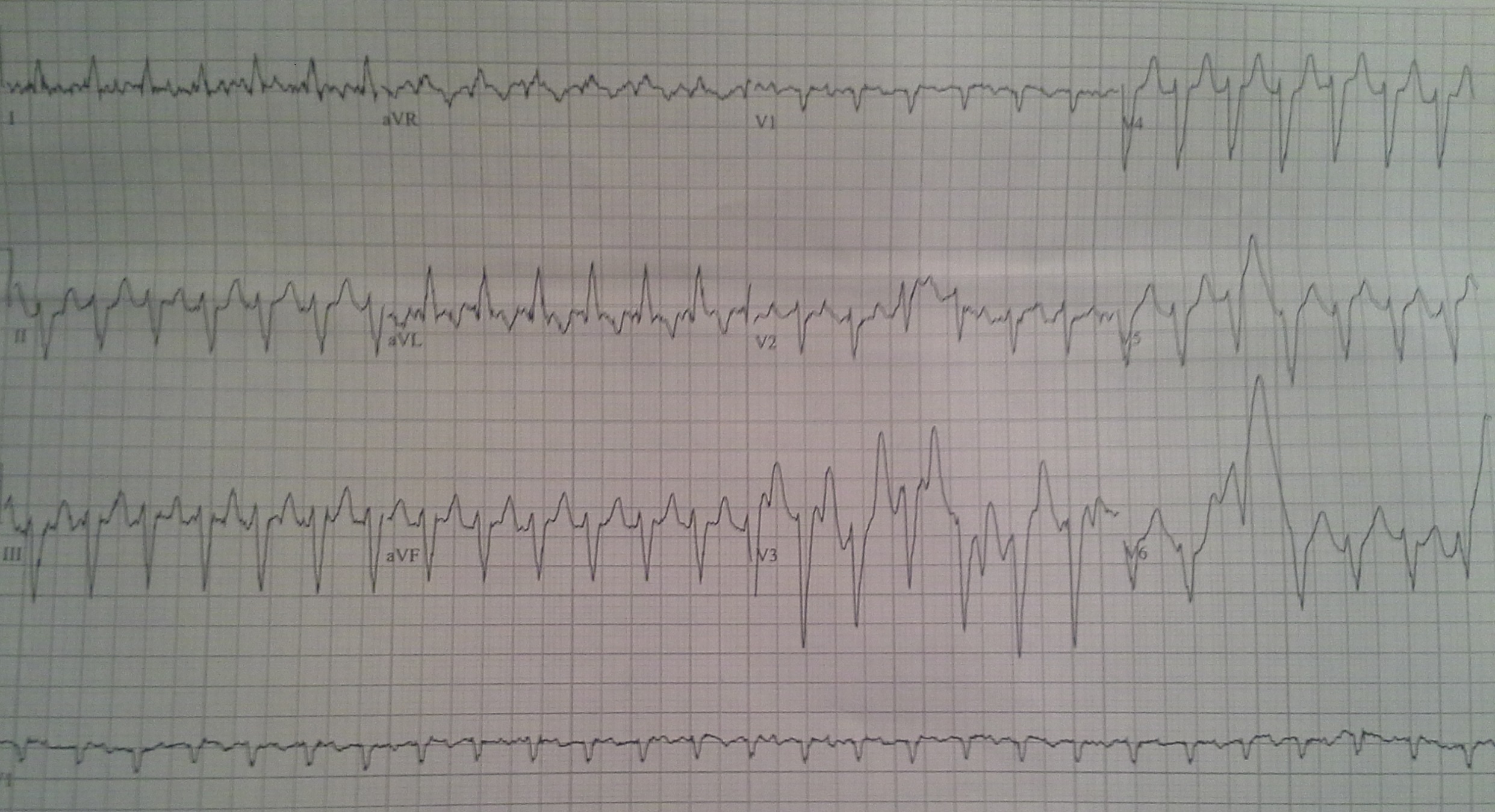
There is an AV dissociation where the P waves march out.
There is a slightly wide QRS, but not that wide.
There is a small variability in the morphology of the QRS complexes.
All of these factors taken together lead to one of several options:
- AV dissociation with accelerated junctional rhythm
- Rare, unlikely as this patient was not on digoxin but not impossible
- Ventricular tachycardia with AV dissociation
- Idiopathic ventricular tachycardia difficult to diagnose
- Fascicular VT (narrow QRS 100-140 msec)
- Posterior fascicular 90-95% of the time, RBBB morphology with left axis deviation
- Anterior fascicular 5-10%, LBBB morphology with right axis deviation or inferior deviation
- Isorhythmic AV dissociation
- Another rare form of AV dissociation – sinus P waves and narrow QRS complexes where one beat is conducted and the next beat is an accelerated junctional beat at the same pace had the sinus beat been conducted
- Yet another rhythm?
Of these rhythms, several will respond to adenosine and Fascicular VT will often respond to verapamil. Our ECG has predominantly left bundle branch morphology and an inferior axis which may lend itself to anterior fascicular block and less likely accelerated junctional rhythm.
Remember our patient had this fast “AVNRT” rhythm (seen below) that “broke” into our rhythm in question after adenosine:
So while the best answer now is some form of VT with AV dissociation, possible anterior fascicular VT, further EP studies are needed to definitively diagnose this rhythm. Further discussion is welcome!
References:
Lifeinthefastlane.com articles on: RVOT, Accelerated Junctional Rhythm and Fascicular Tachycardia
Enyon, CA et al. Fascicular Tachycardia: uncommon or just unrecognized? Emerg Med J 2002;19:477-478
Francis J, et al. Idiopathic Fascicular Ventricular Tachycardia. Indian Pacing Electrophysiol J. 2004 Jul-Sep; 4(3): 98–103.
Mattu A, Brady W. ECGs for the Emergency Physician 2, BMJ Books 2008
eabram
Latest posts by eabram (see all)
- Rhythm Nation May 2015 Answer! - June 1, 2015
- Rhythm Nation May 2015 - May 10, 2015
- Rhythm Nation April 2015 – Answer! - April 20, 2015
- Rhythm Nation April 2015 - April 13, 2015
- Rhythm Nation March 2015 – Answer! - March 31, 2015
3 comments for “Rhythm Nation February 2015 – Answer”