
26 yo M pmh multiple episodes of syncope as child p/w anxiety symptoms for months. No meds or illicits. His father died at age 39.
He has the following dysrhythmia:
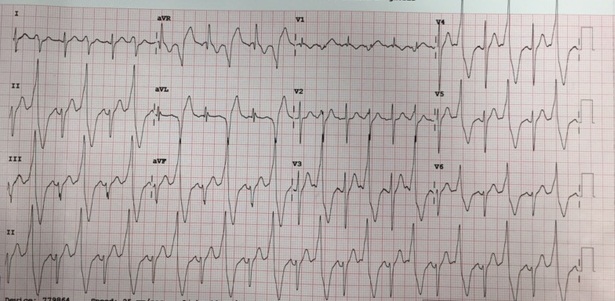
Questions:
What is this rhythm?
What is your ED care and dispo?
Best answer by March 23 at noon is our winner.
Special note, the ECG was flipped right side up after VTACHomas’ comment below.
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

eabram
Latest posts by eabram (see all)
- Rhythm Nation May 2015 Answer! - June 1, 2015
- Rhythm Nation May 2015 - May 10, 2015
- Rhythm Nation April 2015 – Answer! - April 20, 2015
- Rhythm Nation April 2015 - April 13, 2015
- Rhythm Nation March 2015 – Answer! - March 31, 2015
3 comments for “Rhythm Nation March 2015”