
The Case
7 year old Hispanic male presents to an imaginary ED with complaints of “heart racing” for one day. He has a known history of HTN and is on metoprolol. Parents are unsure of other cardiac history.
VS: HR: 166, RR: 17, BP: 111/86, Temp: 98 F, SaO2- 100%
Exam is normal.
EKG (no previous):
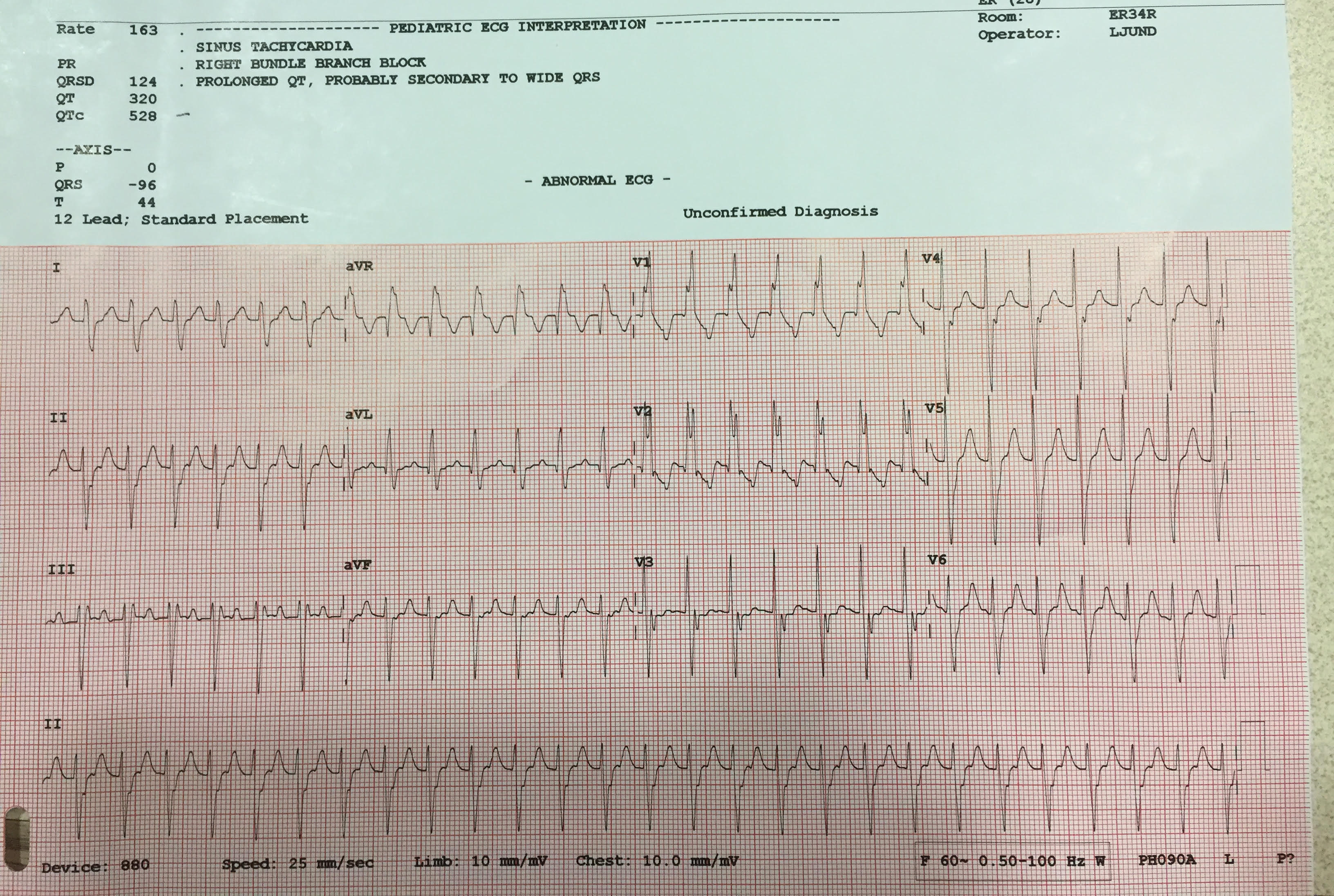
What is the Diagnosis?
Ventricular Tachycardia- specifically Belhassen’s Tachycardia or Idiopathic Fascicular Ventricular Tachycardia. This is a reentry ventricular tachycardia mediated through calcium channel-conduction pathways. It typically occurs in patients ages 15-40 with a structurally NORMAL heart (hence, idiopathic). Reports are present in younger children and infants! Parents are hopefully given a card listing this diagnosis as it is probably very hard for them to remember.
Attacks may be caused by exercise, excitement, or infection. Patients usually present with palpitations or vague complaints but are typically hemodynamically stable. The prognosis is excellent and sudden death is rare.
One of the first descriptions of this disease was by Belhassen in 1984. Classically it is described as
- right bundle branch block pattern
- left axis deviation
- QRS duration of around 120 msec
The above findings describe the most common type of Bellhassen Tachycardia- arising from the posterior fascicle in the left ventricle (90-95% of cases). Anterior Fascicle V-tach will give you a Right bundle block branch pattern with right axis deviation which is what our patient has.
Differential diagnosis for this case include: regular SVT with rate-related aberrancy and regular SVT with RBBB. It is very hard to distinguish this on the EKG presented. Parents luckily gave a business card with the diagnosis of “Bellhassen Ventricular Tachycardia” and this helped with the management.
What is the management?
Keep in mind no response to adenosine suggests VT. If the rhythm was to terminate with adenosine that means it has a reentry circuit that involves the AV node. A transient AV block may be diagnostic in some cases and reveal flutter waves, MAT, atrial tachycardia, or even sinus tachycardia. Regardless, PALS does suggest adenosine for Stable VT (like this patient).
Vagal maneuvers could be attempted, though there may be no response. The next management step used was IV procainamide was attempted (15 mg/kg over 30 minutes) without success. IV verapamil (0.075-0.15 mg/kg (max 10 mg) IV over 2 minutes) was given – this terminated the VT and patient reverted to normal sinus rhythm.
Conclusion
By Dr. Jacqueline Bober
Special Thanks to Dr. Ian deSouza for his timely, thorough, and very helpful feedback
References
Prystowsky EN et al. Ventricular Arrhythmias in the Absence of Structural Heart Disease. American College Of Cardiology. 2012;59(20)”1733-1744
Quimby et al. Idiopathic Ventricular Tachycardia: Belhassen Type. 2010 West J Emerg Med. 2010; 11(4):389-390
http://lifeinthefastlane.com/ecg-library/fascicular-vt/
Belhassen et al. Idiopathic recurrent sustained ventricular tachycardia responsive to verapamil: an ECG-electrophysiologic entity. Am Heart J. 1984 Oct; 108(4 Pt 1): 1034-7
http://www.heartpearls.com/tag/posterior-fascicular-ventricular-tachycardia
http://www.cardiophile.com/idiopathic-fascicular-ventricular-tachycardia-belhassens-ventricular-tachycardia/
Wang et al. Verapamil Sensitive Idiopathic Ventricular Tachycardia in an Infant. Japanese Heart Journal
Vol. 44 (2003) No. 5 P 667-671
andygrock
- Resident Editor In Chief of blog.clinicalmonster.com.
- Co-Founder and Co-Director of the ALiEM AIR Executive Board - Check it out here: http://www.aliem.com/aliem-approved-instructional-resources-air-series/
- Resident at Kings County Hospital
Latest posts by andygrock (see all)
- A Tox Mystery…. - May 26, 2015
- Of Course, US Only for Kidney Stones… - May 18, 2015
- Case of the Month 11: Answer - May 12, 2015
- Too Classic a Question to Be Bored Review - May 5, 2015
- Case of the Month 11: Presentation - May 1, 2015