
20 year old muscular 6’3″ man presents to the ED with chest pain and states that it feels like “bubble wrap popping” when he bends over and reports some difficulty breathing. No hx of trauma. You get a CXR and see: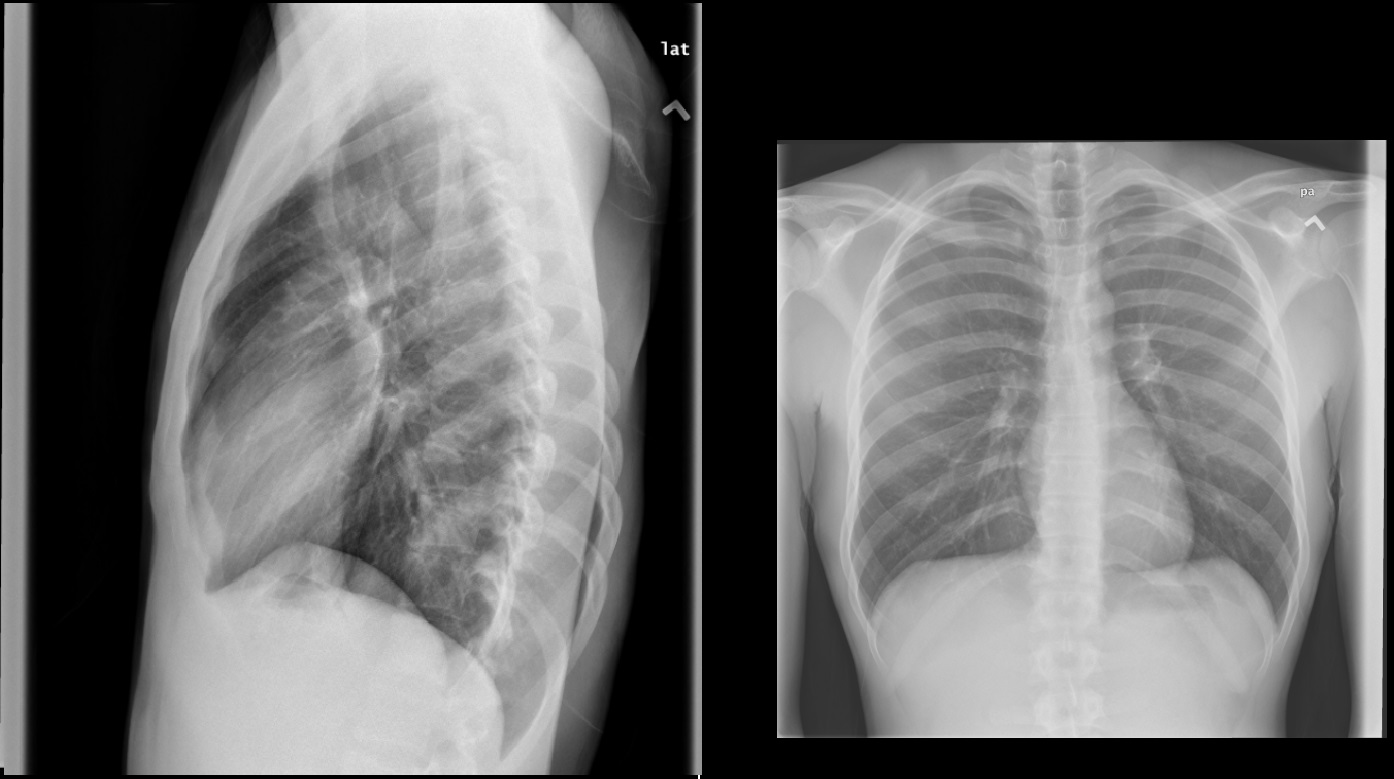
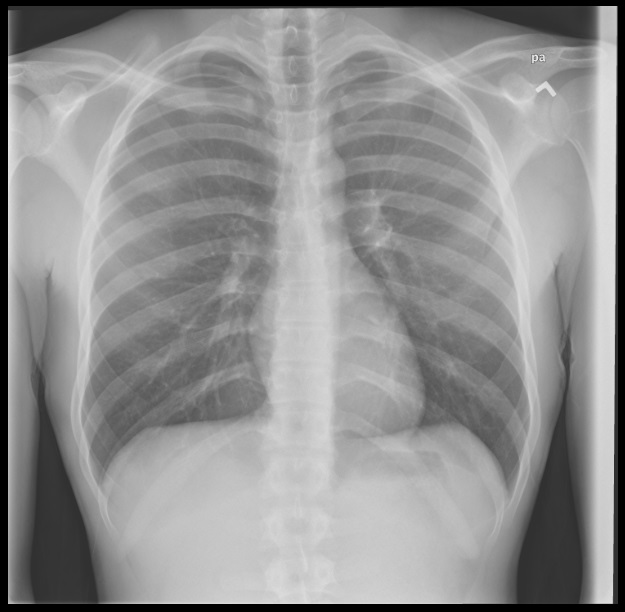
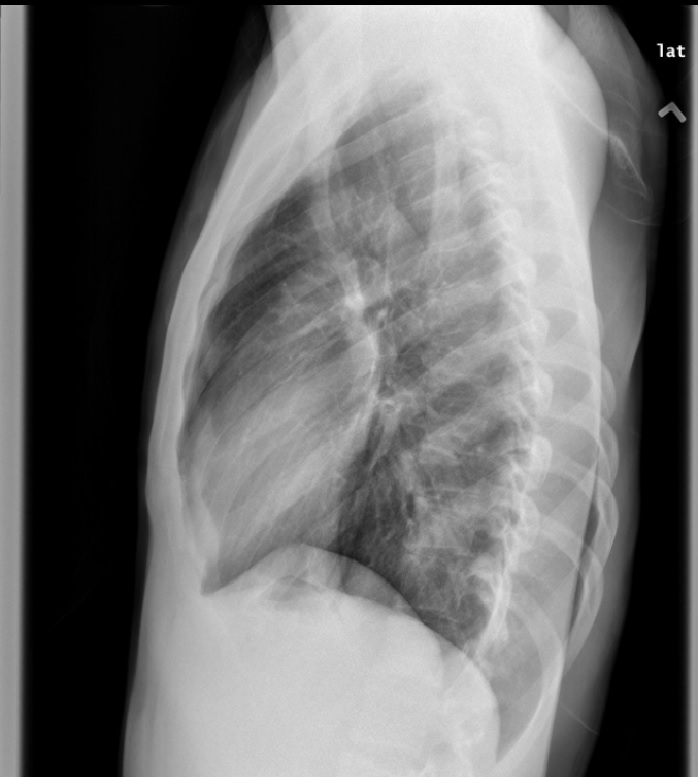 Vitals: BP 110/80, HR 105, RR 22, O2 sat 95% on RA, afebrile. What does he have and how would you manage this?
Vitals: BP 110/80, HR 105, RR 22, O2 sat 95% on RA, afebrile. What does he have and how would you manage this?
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

sliang
EM-IM Resident at SUNY Downstate/Kings County Hospital
Latest posts by sliang (see all)
- Xray Vision: Chest Pain Answer - June 26, 2015
- Xray Vision: Chest Pain - June 14, 2015
4 comments for “Xray Vision: Chest Pain”