
Presented by: Dr. Andrew Nguyen
Summarized by: Dr. Wendy Chan
Reviewed by: Dr. Ian deSouza
The Fictitious Case: 81 y/o F with PMH HTN, DM, CVA, afib, CAD, and recent hospitalization presents with 1 week of generalized weakness, nausea w/o vomiting, and pain to left toes with swelling and discoloration. Her triage vital signs and fingerstick were within normal range. Physical exam was significant for “awake but lethargic” mental status, left-sided weakness, an irregularly irregular heartbeat, and left first through fourth digit erythema, edema, and fluctuance with palpable pulse. Labs were significant for anemia, thrombocytopenia, hyperkalemia, elevated PT/INR and PTT, elevated BNP, elevated Cr, and mildly elevated troponin. U/A + many bacteria and WBCs. Lactate 9.1.
The patient was fluid resuscitated and antibiosed. ED team suspected TTP given anemia, thrombocytopenia, elevated creatinine, and altered mental status. Hematology was consulted and agreed with the diagnosis of TTP, and management was to include plasmapheresis; however after patient was transferred to the MICU, the fibrinogen labwork returned significantly reduced with an elevated D-Dimer and the diagnosis was revised to DIC. (fibrinogen levels are normal in TTP) Patient was transfused with 10 units of cryoprecipitate. On hospital day #6 patient arrested and was pronounced.
Cause of death presumed to be DIC secondary to MODS (multiple organ dysfunction syndrome) secondary to global microvascular thrombosis with subsequent ischemia and inflammation. Sepsis was not thought to be the cause of death because the patient was appropriately antibiosed and her lactate trended towards normal over hospital course (Lactate 9.1 –> 2.6)
Pathophysiology of DIC is a consumptive coagulopathy.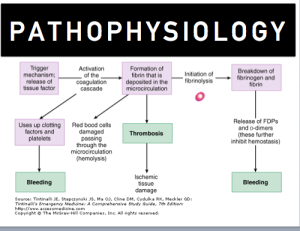
Tissue factor is activated by an inciting insult, such as severe sepsis, trauma, or malignancy. The tissue factor triggers the coagulation cascade which leads to 1) thrombosis due to fibrin deposits and then later a hyperfibrinolysis which leads to fibrinogen depletion and bleeding 2) bleeding due to thrombocytopenia and depletion of clotting factors.
Diagnosis of DIC is primarily made by laboratory findings of coagulation derangements in context of of recent inciting incident known to cause DIC
-Elevated PT/INR and PTT
-Initially normal fibrinogen, then decreased during the “consumption” phase
-Thrombocytopenia
-Elevated D-dimer or other fibrinogen degradation products (I.E. thrombomodulin)
-Possible schistocytes on peripheral smear
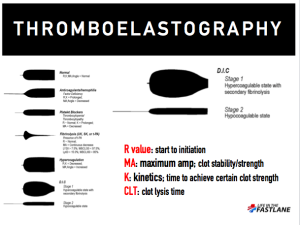
-Future diagnosis of DIC may include point-of-care tests like thromboelastography (TEG)
Signs and Symptoms of DIC- bleeding is hallmark, multiple organ injury is secondary
-64% of patients will have abnormal bleeding
-Organ dysfunction is a result of the widespread thrombosis in the microcirculation. Kidney, liver, and lungs are the most common organs affected
Treatment is targeted at fixing the underlying cause
-Transfuse pRBCs as needed for anemia, bleeding, or planned invasive procedure
- Consider platelets in the 20k-50k range
- FFP- however lacks factor VII, inadequate choice for transition
- PCC (II, VII, IX, X, Protein C, S)- however lacks important extrinsic pathway factors, inadequate choice for transition
- Cryoprecipitate to replete fibrinogen
- Vitamin K
- Use of anticoagulants and antifibrinolytics such as heparin and tranexamic acid respectively are not recommended due to lack of evidence
- Antithrombin and thrombomodulin show promise reducing DIC scores, further studies needed
- Activated Protein C was previously recommended however the guidelines were changed and it was withdrawn from the market in 2011
Conclusions
-Broad differential
-Consider DIC early in course of great physiologic insult
-End organ damage global, appreciate physical exam
-Use lab studies as guide in diagnosis
-Treat underlying cause
-Transfuse for bleeding, consider TEG as guide
-Anticoagulation has been traditionally used, mortality benefit unclear, larger numbers to appreciate harm
-Novel therapies (namely thrombomodulin) may be more beneficial when provided early in course
Resources
Gando S, Saitoh D, Ishikura H, Ueyama M, Otomo Y, Oda S, et al. A randomized, controlled, multicenter trial of the effects of antithrombin on disseminated intravascular coagulation in patients with sepsis. Critical Care 2013;17(6):R297
Liu XL, Wang XZ, Liu XX, Hao D, Jaladat Y, Lu F, Sun T, Lv CJ. Low-dose heparin as treatment for early disseminated intravascular coagulation during sepsis: a prospective clinical study. Exp Ther Med. 2014;7:604–608.
Pernerstorfer T, Hollenstein U, Hansen J, Knechtelsdorfer M, Stohlawetz P, Graninger W, et al. (1999) Heparin blunts endotoxin-induced coagulation activation. Circulation 100: 2485–2490.
Semeraro, Nicola, Concetta T. Ammollo, Fabrizio Semeraro, and Mario Colucci. “Sepsis-Associated Disseminated Intravascular Coagulation And Thromboembolic Disease.” Mediterranean Journal of Hematology and Infectious Diseases Mediterr J Hematol Infect Dis 2.3 (2010): 2010024. Web.
Thachil J, Toh CH, Levi M, Watson HG. The withdrawal of Activated Protein C from the use in patients with severe sepsis and DIC [Amendment to the BCSH guideline on disseminated intravascular coagulation]. Br J Haematol 2012;157:493–4.
Tomoaki Y, Nakamura R, Kumagai N, Iilyama T, Tamashita K, Yokoyama M. Administration of recombinant thrombomodulin before progression of disease causing disseminated intravascular coagulation might be better compared with administration after progression of disease. Journal of Intensive Care. 2014. 2;49.
Wada H, Matsumoto T, Yamashita Y: Diagnosis and treatment of disseminated intravascular coagulation (DIC) according to four DIC guidelines.Journal of Intensive Care 2014, 2:15.
wendyrollerblades
Latest posts by wendyrollerblades (see all)
- EM-CCM Hematology 7/22/2015:Treating DIC - July 27, 2015
- Critical Care: Recent Trials in Sepsis - May 1, 2015
- TASER Conducted Electrical Weapon Injuries - March 9, 2015
- Racially Biased Pain Control in the ED - December 15, 2014
- Cyra Whaa?!: Cautionary Tales About ER Folks Who Didn’t Use Skilled Translators - September 22, 2014