
Thanks to Dr. Wang for today’s Morning Report!
Lateral Orbital Canthotomy
Indications:
- Retrobulbar hemorrhage
- Increase IOP (IOP >40mm Hg)
- Proptosis
Contraindications:
- Globe rupture
- Hyphema
- Tear-drop-shaped pupil
- Peaked or irregularly shaped pupil
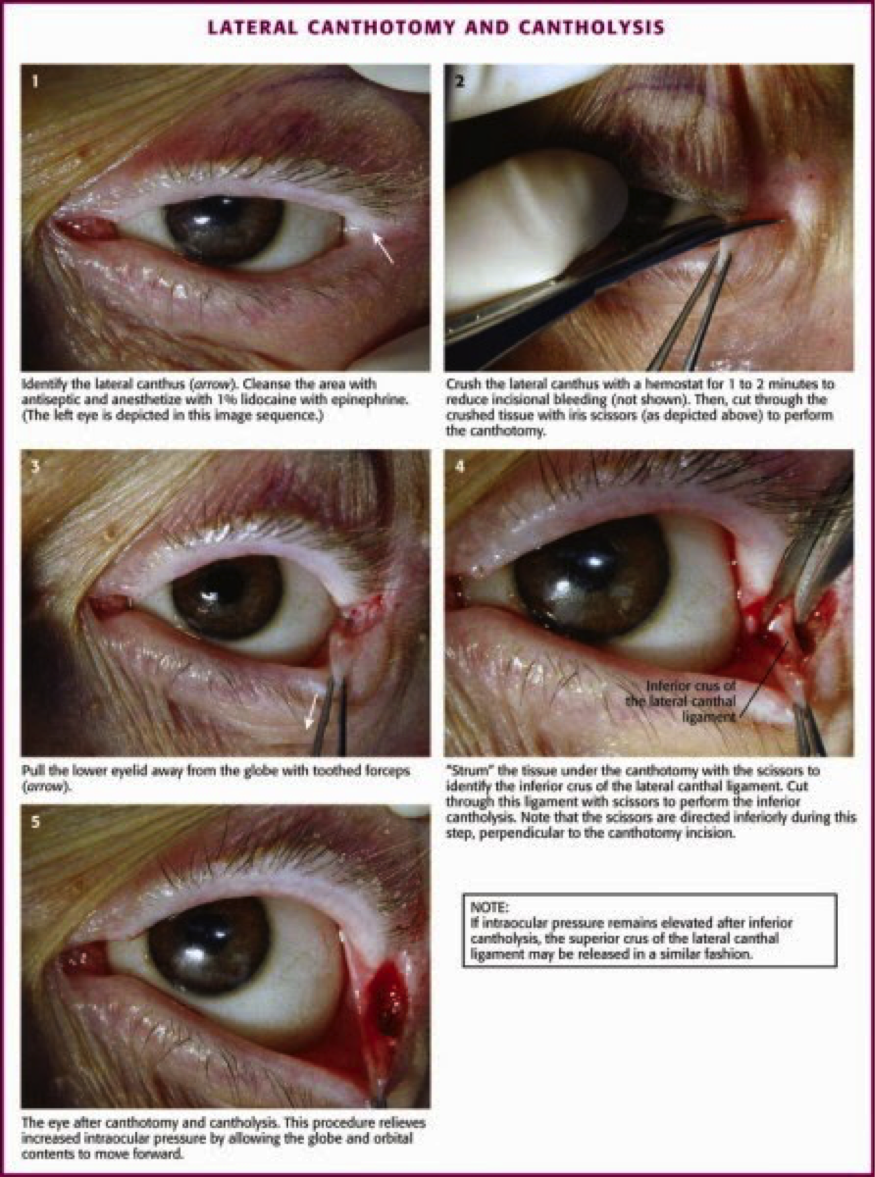
Procedure:
- Positioning: patient in the supine position. Possibly restrained or undergo conscious sedation
- Local anesthesia (lidocaine 1-2% with epinephrine) is injected into the lateral canthus. Direct need tip toward the lateral orbital rim and begin injecting when the needle hits bone.
- Irrigate the affected eye of debris with normal saline
- Use the hemostat to clamp the skin at the lateral corner of the patient’s eye for 1-2 mins. Helps to achieve hemostasis and mark the location where the incision is to be made.
- Use forceps to pick up the skin around the lateral orbit
- Use scissors to make a 1-2 cm incision beginning at the lateral corner of the eye and extending laterally outward
- Retract the inferior lid downward to visualize the lateral canthus tendon
- Direct scissors along lateral orbital rim
- If IOP remains > 40mm Hg, cut superior portion of the lateral tendon by dissecting superiorly before cutting it
- Successful procedure is marked by improved visual acuity and decrease of IOP to below 40mm Hg.
References:
http://emedicine.medscape.com/article/82812-overview
http://www.emcurious.com/blog-1/2014/9/25/the-lateral-canthotomy
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.




Jay Khadpe MD
Editor in Chief of "The Original Kings of County"
Assistant Professor of Emergency Medicine
Assistant Residency Director
SUNY Downstate / Kings County Hospital
Latest posts by Jay Khadpe MD (see all)
- Morning Report: 7/30/2015 - July 30, 2015
- Morning Report: 7/28/2015 - July 28, 2015
- IN THE STRETCHER INSTEAD OF BESIDE IT - July 22, 2015
- Morning Report: 7/14/2015 - July 14, 2015
- Morning Report: 7/10/2015 - July 10, 2015