

http://phil.cdc.gov/phil/details.asp?pid=3168
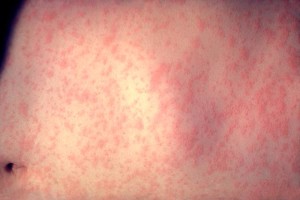
A 2 year-old boy presents to your ED with a history of 7 days of tactile temperatures and a rash. The rash started on day 3 of the fever and now has spread to the whole body. The child is from the Caribbean and has not received any vaccines since six months of age. The child has been healthy otherwise. They came to your ED for further evaluation. Vitals in the ED are within normal limits. Exam is significant for the rash above, erythematous pharynx, and slightly injected conjunctivae. There is no murmur, no abdominal masses, and the child is non-toxic appearing.
Upon seeing this rash, what should be included in your differential?Dengue Fever
Measles
Kawasaki’s Disease
Group A strep
Other viruses including Coxsackie, Rubella
Drug Reaction
What is the most likely diagnosis given the history above?
Measles
What you need to know:
- The vaccine is typically given in the US at age 12 months.
- The 3 C’s- Cough/Coryza/Congestion. . . This is the prodrome- it will occur before the rash starts and can continue for 7-8 days and usually is accompanied by high fevers.
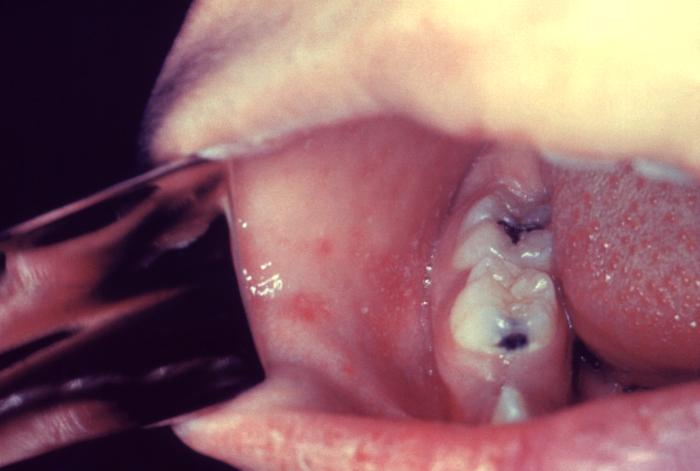
- Koplik spots: they were not seen in this child’s mouth. If the child has the rash, you will NOT see them. They occur prior to the rash and last about 36-72 hours. They are usually along the buccal mucosa and are red spots with whitish/bluish centers.
 http://phil.cdc.gov/phil/details.asp?pid=3168
http://phil.cdc.gov/phil/details.asp?pid=3168 - The RASH: Starts on head and usually spreads downward- sparing the palms and soles. It fades in the same direction. Usually starts in the mid-disease. Pharyngitis and fever can accompany this rash. If fever is persisting past 3-4 days of the rash—think of measles associated complications.
- Complications:
- Most common: diarrhea
- Scariest: Encephalitis (high rate of neurologic damage) or Pneumonia
- Pneumonia or lung related infections are the leading cause of death in children (can be from measles virus or secondary infection)
If you are considering a patient may have measles:
- CALL INFECTION CONTROL- precautions need to be used for proper room cleaning and how to approach a patient. The virus is spread via respiratory droplets and airborne. Airborne transmission precautions are indicated for 4 days after the onset of rash in otherwise healthy children
- Order serum IgM for Measles antibody- these usually appear on Day 3 of the rash and last up to 30 days
- You may need to admit depending on typical severity of illness or if Kawasaki’s is top differential
- Support any of the complications. Vitamin A is recommended for treatment of any patients with acute Measles and should be discussed with Infectious Disease Team.
By: Jackie Bober
References:
Zenel, JA.Visual Diagnosis: An Infant Who Has Fever and Rash. Pediatrics in Review 2000;21;105
Centers for Disease Control and Prevention. Summary of notifiable diseases, United States, 1997. MMWR. 1998;46(54):6
RED BOOK®: 2012 REPORT OF THE COMMITTEE ON INFECTIOUS DISEASES – 29th Ed. (2012). Measles
PEM FELLOWS
Latest posts by PEM FELLOWS (see all)
- Not your typical rash . . . - July 13, 2015
1 comment for “Not your typical rash . . .”