
Written by Dr. Michelle DiMare
Welcome back! This month’s post is brought to you by my sudden increase in peds shifts and everyone’s favorite chief complaint: vomiting.
While ultrasounding a tiny, crying, puking, squirmy patient can often seem like a daunting task, this post will hopefully help you hit your target… please forgive that terrible joke.
Because of the sheer number of generally healthy appearing children we see with a complaint of vomiting, it is often difficult to weed out the few that may be in the early stages of a critical illness. Bedside ultrasound can aid in early detection in two cases in particular: pyloric stenosis and intussusception. This post will address bedside ultrasound for pyloric stenosis.
Though pyloric stenosis can lead to severe dehydration early on, children often present with brief episodes of extreme symptoms intermixed with the patient appearing happy and hungry.
The Target: Pyloric Stenosis

- Infants in the first 3 months of life
- most often around 3 weeks
- Males more than females in a 4:1 ratio
- Projectile vomiting in an otherwise hungry appearing baby
- Place baby in mom or dad’s lap
- Avoid feeding prior to US as bowel gas can obscure images
- Allow to breast or bottle feed a small amount during the ultrasound to soothe the baby
- Position the baby just slightly raised from supine, left side tilted up
- This will help direct feeds through pylorus and air away from it
- “Mow the lawn” as pictured below
- Scan the whole abdomen in an organized pattern looking for grossly abnormal pathology

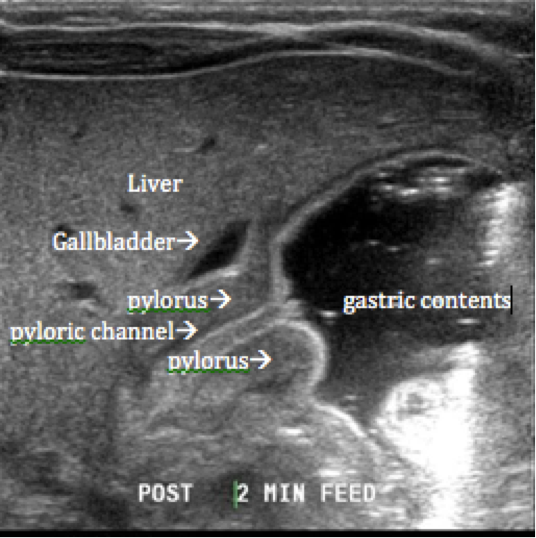
- Localize to the epigastric area, looking for the liver and the gallbladder
- With pyloric stenosis, the pylorus is often displaced just inferior and adjacent to the gallbladder
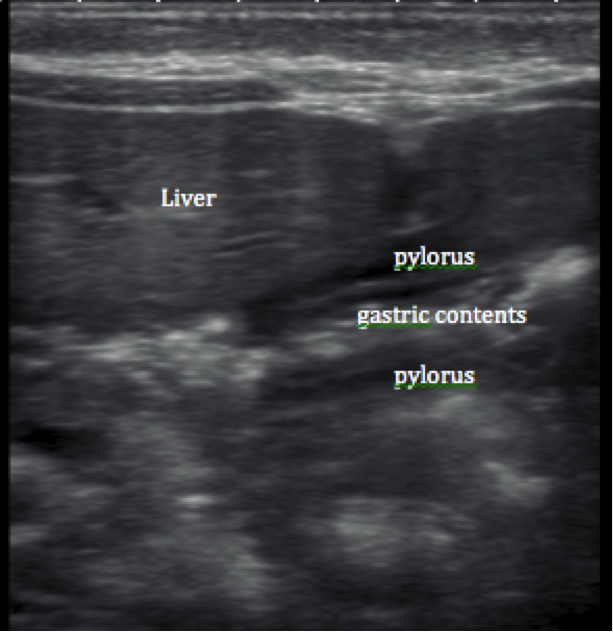
What are you looking for?
Normal:
Hypertrophic Pyloric Stenosis:
- No gastric contents freely passing through the canal
- Hypertrophic pylorus with a single muscle wall measuring >3mm on transverse view
- Pyloric canal measuring >14 mm
Antral Nipple:
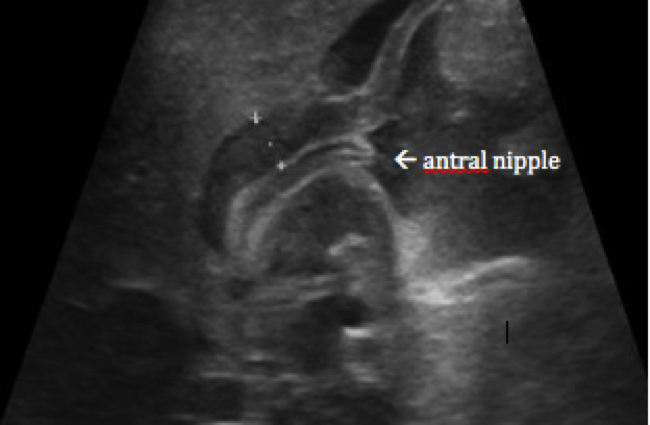
- Redundant pyloric mucosa protruding into the gastric antrum
Though rare, pyloric stenosis is worth considering in all patients under three months of age with persistent projectile vomiting. Finding the one abnormal case will be much easier if you’ve scanned and seen your fair share of normal anatomy.
Thanks for reading my last post as a fellow. As always, happy scanning!
jshibata
- Resident Editor-in-chief of blog.clinicalmonster.com
- Blog author of kchemimage.wordpress.com/category/clinical-radiographs/
- Co-author of the Resident Journal Review for AAEM’s Common Sense newsletter.
- EM/IM Resident at Kings County Hospital
Latest posts by jshibata (see all)
- Tox Craze - July 30, 2015
- PE or not PE, that is the question… - July 29, 2015
- Right on Target: A Petite Peds Post - July 6, 2015
- ARVD/C - June 18, 2015
- A dose of primary care for hyperglycemia in the ED: optimizing the discharge. - May 5, 2015