
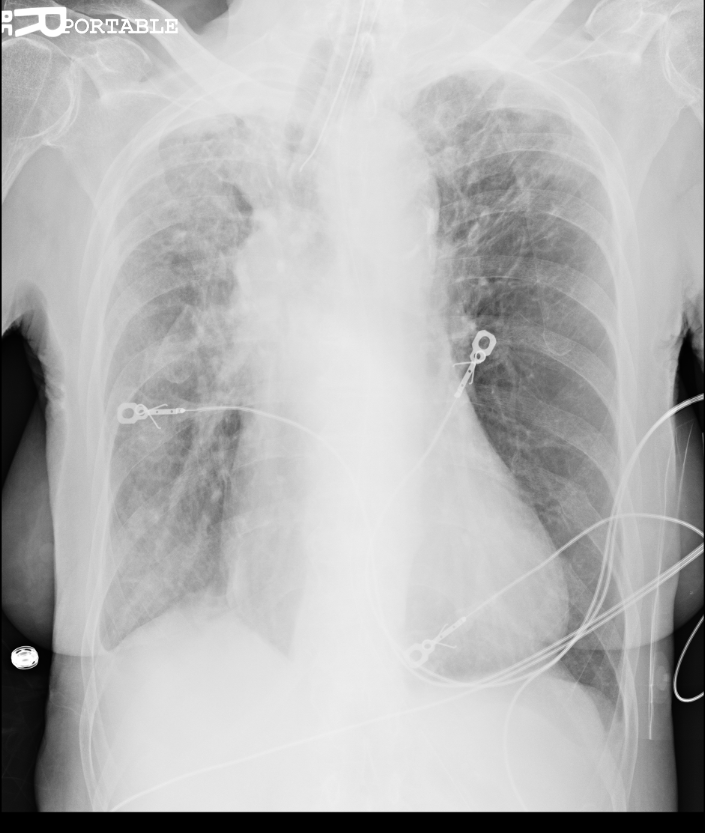
Here is a case where most to all of the medical history could be obtained from the chest x-ray. Patient is an 81 yo W found apneic and cyanotic and EMS was called and patient was intubated. Patient had never been here before and no history came with the patient. The history was obtained with this chest x-ray.
Read the chest x-ray in formal layout for gift card.
Let me know you thoughts and your care for the patient.
The views expressed on this blog are the author's own and do not reflect the views of their employer. Please read our full disclaimer here. Any references to clinical cases refer to patients treated at a virtual hospital, Janus General Hospital.
The following two tabs change content below.

mritchie
Latest posts by mritchie (see all)
- X-ray Vision: The answer - July 31, 2013
- X-ray Vision: Ortho - July 17, 2013
- X-ray Vision Answer: - April 17, 2013
- X-ray Vision: Stories in the chest x-ray - April 2, 2013
- Rhythm Nation: Case 6 Answer - March 23, 2013
4 comments for “X-ray Vision: Stories in the chest x-ray”